

The sequential trauma score - a new instrument for the sequential mortality prediction in major trauma
- PMID: 20562057
- PMCID: PMC3352007
- DOI: 10.1186/2047-783x-15-5-185
The sequential trauma score - a new instrument for the sequential mortality prediction in major trauma
Abstract
Background: There are several well established scores for the assessment of the prognosis of major trauma patients that all have in common that they can be calculated at the earliest during intensive care unit stay. We intended to develop a sequential trauma score (STS) that allows prognosis at several early stages based on the information that is available at a particular time.
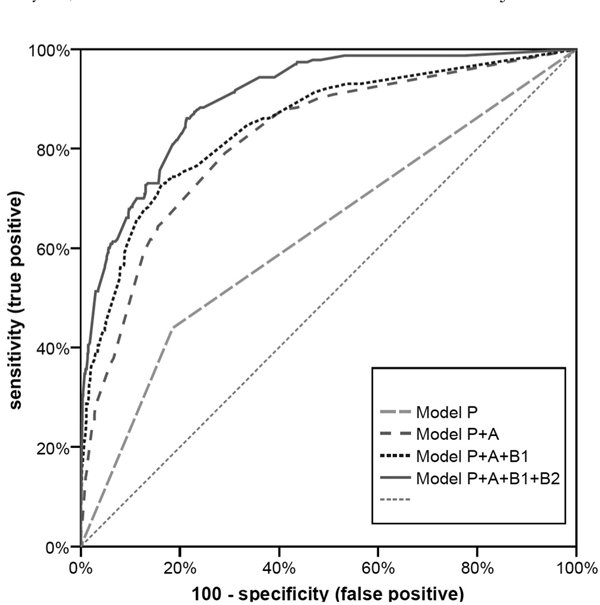
Study design: In a retrospective, multicenter study using data derived from the Trauma Registry of the German Trauma Society (2002-2006), we identified the most relevant prognostic factors from the patients basic data (P), prehospital phase (A), early (B1), and late (B2) trauma room phase. Univariate and logistic regression models as well as score quality criteria and the explanatory power have been calculated.
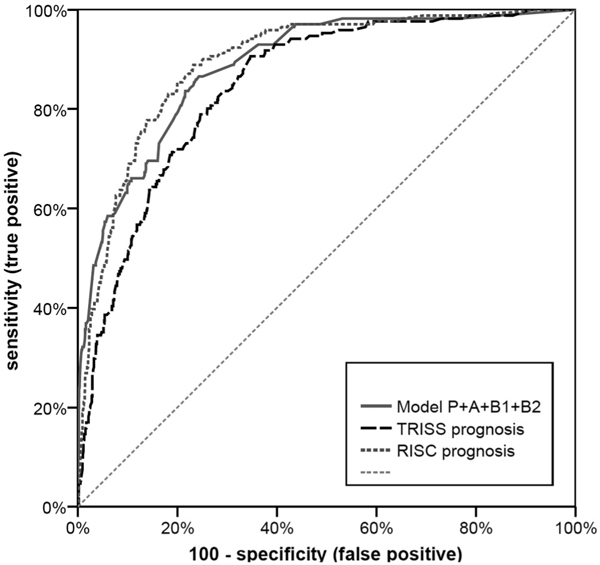
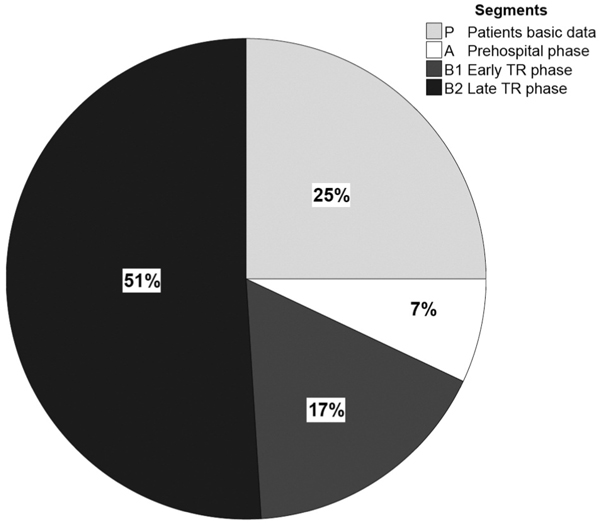
Results: A total of 2,354 patients with complete data were identified. From the patients basic data (P), logistic regression showed that age was a significant predictor of survival (AUC(model P), area under the curve = 0.63). Logistic regression of the prehospital data (A) showed that blood pressure, pulse rate, Glasgow coma scale (GCS), and anisocoria were significant predictors (AUC(model A) = 0.76; AU(model P + A) = 0.82). Logistic regression of the early trauma room phase (B1) showed that peripheral oxygen saturation, GCS, anisocoria, base excess, and thromboplastin time to be significant predictors of survival (AUC(model B1) = 0.78; AUC(model P + A + B1) = 0.85). Multivariate analysis of the late trauma room phase (B2) detected cardiac massage, abbreviated injury score (AIS) of the head > or = 3, the maximum AIS, the need for transfusion or massive blood transfusion, to be the most important predictors (AUC(model B2) = 0.84; AUC(final model P + A + B1 + B2) = 0.90). The explanatory power - a tool for the assessment of the relative impact of each segment to mortality - is 25% for P, 7% for A, 17% for B1 and 51% for B2. A spreadsheet for the easy calculation of the sequential trauma score is available at: www.sequential-trauma-score.com
Conclusions: This score is the first sequential, dynamic score to provide a prognosis for patients with blunt major trauma at several points in time. With every additional piece of information the precision increases. The medical team has a simple, useful tool to identify patients at high risk and to predict the prognosis of an individual patient with major trauma very early, quickly and precisely.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
