

The Relationship among Hypoxia, Proliferation, and Outcome in Patients with De Novo Glioblastoma: A Pilot Study
- PMID: 20563257
- PMCID: PMC2887645
- DOI: 10.1593/tlo.09265
The Relationship among Hypoxia, Proliferation, and Outcome in Patients with De Novo Glioblastoma: A Pilot Study
Abstract
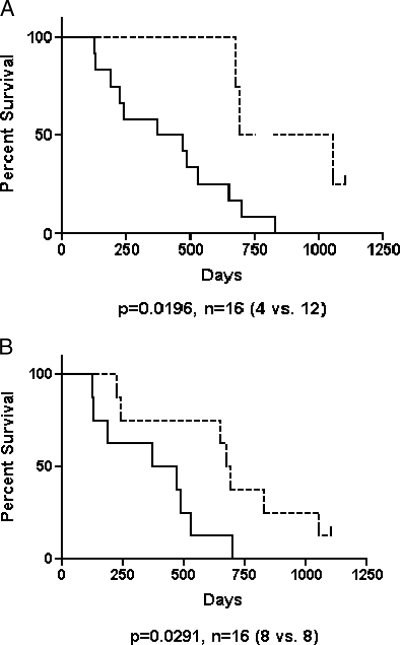
The hypoxia and proliferation index increase with grade in human glial tumors, but there is no agreement whether either has prognostic importance in glioblastomas. We evaluated these end points individually and together in 16 de novo human glioblastomas using antibodies against the 2-nitroimidazole hypoxia detection agent EF5 and the proliferation detection agent Ki-67. Frozen tumor tissue sections were fluorescence-stained for nuclei (Hoechst 33342), hypoxia (anti-EF5 antibodies), and proliferation (anti-Ki-67 antibodies). EF5 binding adjacent to Ki-67+ cells, overall EF5 binding, the ratio of these values, and the proliferation index were evaluated. Patients were classified using recursive partitioning analysis and followed up until recurrence and/or death. Recursive partitioning analysis was statistically significant for survival (P = .0026). Overall EF5 binding, EF5 binding near Ki-67+ cells, and proliferation index did not predict recurrence. Two additional survival analyses based on ratios of the overall EF5 binding to EF5 binding near Ki-67+ cells were performed. High and low ratio values were determined by two cutoff points: (a) the 50% value for the ratio [EF5/Ki-67(Binding)]/[Tumor(binding)] = Ratio(EF5 50%) and (b) the median EF5 value (75.6%) of the ratio [EF5/Ki-67(Binding)]/[Tumor(binding)] = Ratio(patients median). On the basis of the Ratio(EF5 50%), recurrence (P = .0074) and survival (P = .0196) could be predicted. Using the Ratio(patients median), only survival could be predicted (P = .0291). In summary, patients had a worse prognosis if the [EF5/Ki-67(Binding)]/[Tumor(binding)] ratio was high. A hypothesis for the mechanisms and translational significance of these findings is discussed.
Figures




References
-
- Stupp R, Dietrich PY, Ostermann Kraljevic S, Pica A, Maillard I, Maeder P, Meuli R, Janzer R, Pizzolato G, Miralbell R, et al. Promising survival for patients with newly diagnosed glioblastoma multiforme treated with concomitant radiation plus temozolomide followed by adjuvant temozolomide. J Clin Oncol. 2002;20:1375–1382. - PubMed
-
- Wen PY, Kesari S. Malignant gliomas in adults. N Engl J Med. 2008;359:492–507. - PubMed
-
- Brahimi-Horn MC, Chiche J, Pouyssegur J. Hypoxia and cancer. J Mol Med. 2007;85:1301–1307. - PubMed
-
- Evans SM, Koch CJ. Prognostic significance of tumor oxygenation in humans. Cancer Lett. 2003;195:1–16. - PubMed
-
- Shannon AM, Bouchier-Hayes DJ, Condron CM, Toomey D. Tumour hypoxia, chemotherapeutic resistance and hypoxia-related therapies. Cancer Treat Rev. 2003;29:297–307. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources