

Growth patterns and the use of growth hormone in the mucopolysaccharidoses
- PMID: 20563263
- PMCID: PMC2886985
- DOI: 10.3233/PRM-2010-0106
Growth patterns and the use of growth hormone in the mucopolysaccharidoses
Abstract
Short stature is characteristic of patients with mucopolysaccharidosis (MPS) diseases. For children with skeletal dysplasias, such as MPS, it is important to know the natural history of growth. An understanding of the natural growth pattern in each MPS disease provides a measurement to which treatments can be compared, as well as data which can help families and providers make individualized decisions about growth promoting treatments. Multiple advancements have been made in the treatment of MPS with both hematopoietic cell transplantation (HCT) and enzyme replacement therapy (ERT). The long term benefit of these treatments on growth is unknown. This article will review the published data on growth in children with MPS, and describe preliminary data on the use of human growth hormone (hGH) in children with MPS.
Keywords: Growth; MPS; endocrine disease; growth hormone; mucopolysaccharidoses.
Conflict of interest statement
Dr. Polgreen has research support from Genentech. Dr. Miller has research support from Genentech, Pfizer, Norditropin, and Tercica, and is part of the speaker’s bureau for Genentech, Pfizer, and Norditropin. However, the work presented in this manuscript was not supported by any of these growth hormone companies.
Figures
Similar articles
-
Effect of recombinant human growth hormone on changes in height, bone mineral density, and body composition over 1-2 years in children with Hurler or Hunter syndrome.Mol Genet Metab. 2014 Feb;111(2):101-6. doi: 10.1016/j.ymgme.2013.11.013. Epub 2013 Dec 11. Mol Genet Metab. 2014. PMID: 24368158 Free PMC article.
-
Long-term cognitive and somatic outcomes of enzyme replacement therapy in untransplanted Hurler syndrome.Mol Genet Metab Rep. 2017 Sep 27;13:64-68. doi: 10.1016/j.ymgmr.2017.07.012. eCollection 2017 Dec. Mol Genet Metab Rep. 2017. PMID: 28983455 Free PMC article.
-
The use of recombinant human growth hormone in patients with Mucopolysaccharidoses and growth hormone deficiency: a case series.Ital J Pediatr. 2019 Aug 1;45(1):93. doi: 10.1186/s13052-019-0691-1. Ital J Pediatr. 2019. PMID: 31370860 Free PMC article.
-
The natural history of neurocognition in MPS disorders: A review.Mol Genet Metab. 2021 May;133(1):8-34. doi: 10.1016/j.ymgme.2021.03.002. Epub 2021 Mar 11. Mol Genet Metab. 2021. PMID: 33741271 Review.
-
Therapies for the bone in mucopolysaccharidoses.Mol Genet Metab. 2015 Feb;114(2):94-109. doi: 10.1016/j.ymgme.2014.12.001. Epub 2014 Dec 9. Mol Genet Metab. 2015. PMID: 25537451 Free PMC article. Review.
Cited by
-
Prevalence and natural history of gibbus deformity in patients with Hurler syndrome.Neuroradiology. 2024 Nov;66(11):2083-2088. doi: 10.1007/s00234-024-03462-4. Epub 2024 Sep 5. Neuroradiology. 2024. PMID: 39235601
-
Imaging findings of mucopolysaccharidoses: a pictorial review.Insights Imaging. 2013 Aug;4(4):443-59. doi: 10.1007/s13244-013-0246-8. Epub 2013 May 5. Insights Imaging. 2013. PMID: 23645566 Free PMC article.
-
Short stature as a presenting symptom of attenuated Mucopolysaccharidosis type I: case report and clinical insights.BMC Endocr Disord. 2018 Nov 12;18(1):83. doi: 10.1186/s12902-018-0311-x. BMC Endocr Disord. 2018. PMID: 30419879 Free PMC article.
-
Growth in patients with mucopolysaccharidosis type III (Sanfilippo disease).J Inherit Metab Dis. 2014 May;37(3):447-54. doi: 10.1007/s10545-013-9658-3. Epub 2013 Oct 31. J Inherit Metab Dis. 2014. PMID: 24173409
-
Failures of Endochondral Ossification in the Mucopolysaccharidoses.Curr Osteoporos Rep. 2020 Dec;18(6):759-773. doi: 10.1007/s11914-020-00626-y. Epub 2020 Oct 16. Curr Osteoporos Rep. 2020. PMID: 33064251 Free PMC article. Review.
References
-
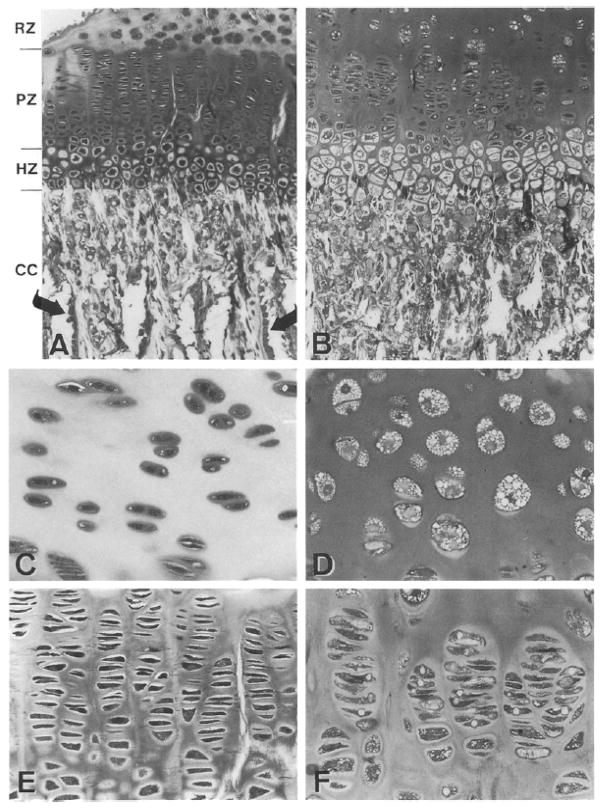
- Abreu S, Hayden J, Berthold P, Shapiro IM, Decker S, Patterson D, Haskins M. Growth plate pathology in feline mucopolysaccharidosis VI. Calcif Tissue Int. 1995;57:185–190. - PubMed
-
- Ali O, Shim M, Fowler E, Greenberg M, Perkins D, Oppenheim W, Cohen P. Growth hormone therapy improves bone mineral density in children with cerebral palsy: a preliminary pilot study. J Clin Endocrinol Metab. 2007;92:932–937. - PubMed
-
- Ali O, Shim M, Fowler E, Cohen P, Oppenheim W. Spinal bone mineral density, IGF-1 and IGFBP-3 in children with cerebral palsy. Horm Res. 2007;68:316–320. - PubMed
-
- Appan S, Laurent S, Chapman M, Hindmarsh PC, Brook CG. Growth and growth hormone therapy in hypochondroplasia. Acta Paediatr Scand. 1990;79:796–803. - PubMed
-
- Argente J, Gracia R, Ibanez L, Oliver A, Borrajo E, Vela A, Lopez-Siguero JP, Moreno ML, Rodriguez-Hierro F. Improvement in growth after two years of growth hormone therapy in very young children born small for gestational age and without spontaneous catch-up growth: results of a multicenter, controlled, randomized, open clinical trial. J Clin Endocrinol Metab. 2007;92:3095–3101. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
