

Long-term results of bariatric restrictive procedures: a prospective study
- PMID: 20563663
- PMCID: PMC2996534
- DOI: 10.1007/s11695-010-0211-2
Long-term results of bariatric restrictive procedures: a prospective study
Abstract
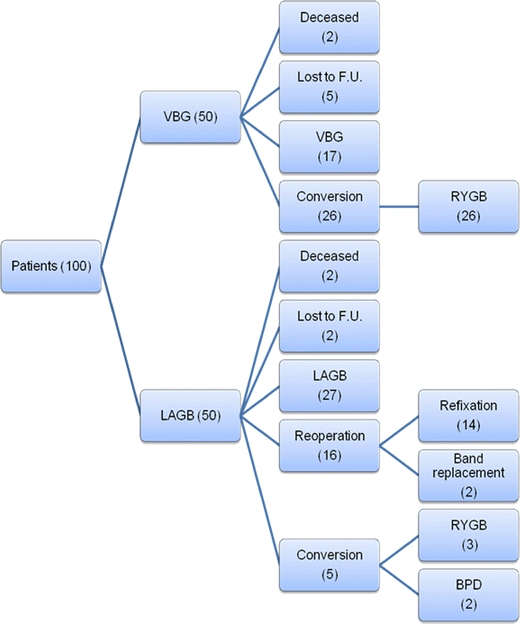
Laparoscopic adjustable gastric banding (LAGB) and vertical-banded gastroplasty (VBG) are surgical treatment modalities for morbid obesity. This prospective study describes the long-term results of LAGB and VBG. One hundred patients were included in the study. Fifty patients underwent LAGB and 50 patients, open VBG. Study parameters were weight loss, changes in obesity-related comorbidities, long-term complications, re-operations including conversions to other bariatric procedures and laboratory parameters including vitamin status. From 91 patients (91%), data were obtained with a mean follow-up duration of 84 months (7 years). Weight loss [percent excess weight loss (EWL)] was significantly more after VBG compared with LAGB, 66% versus 54%, respectively. All comorbidities significantly decreased in both groups. Long-term complications after VBG were mainly staple line disruption (54%) and incisional hernia (27%). After LAGB, the most frequent complications were pouch dilatation (21%) and anterior slippage (17%). Major re-operations after VBG were performed in 60% of patients. All re-operations following were conversions to Roux-en-Y gastric bypass (RYGB). In the LAGB group, 33% of patients had a refixation or replacement of the band, and 11% underwent conversion to another bariatric procedure. There were no significant differences in weight loss between patients with or without re-interventions. No vitamin deficiencies were present after 7 years, although supplement usage was inconsistent. This long-term follow-up study confirms the high occurrence of late complications after restrictive bariatric surgery. The failure rate of 65% after VBG is too high, and this procedure is not performed anymore in our institution. The re-operation rate after LAGB is decreasing as a result of new techniques and materials. Results of the re-operations are good with sustained weight loss and reduction in comorbidities. However, in order to achieve these results, a durable and complete follow-up after restrictive procedures is imperative.
Figures
References
-
- Kemper HC, Stasse-Wolthuis M, Bosman W. The prevention and treatment of overweight and obesity. Summary of the advisory report by the Health Council of The Netherlands. Neth J Med. 2004;62(1):10–7. - PubMed
-
- Bjorntorp P. Results of conservative therapy of obesity: correlation with adipose tissue morphology. Am J Clin Nutr. 1980;33(2 Suppl):370–5. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
