

Population-based analysis of occult primary breast cancer with axillary lymph node metastasis
- PMID: 20564117
- PMCID: PMC4329781
- DOI: 10.1002/cncr.25197
Population-based analysis of occult primary breast cancer with axillary lymph node metastasis
Abstract
Background: Single-institution data suggest that treatment with radiation and axillary lymph node dissection (ALND) may be an appropriate alternative to mastectomy for T0N+ breast cancer. Population-based multi-institutional data supporting this approach are lacking.
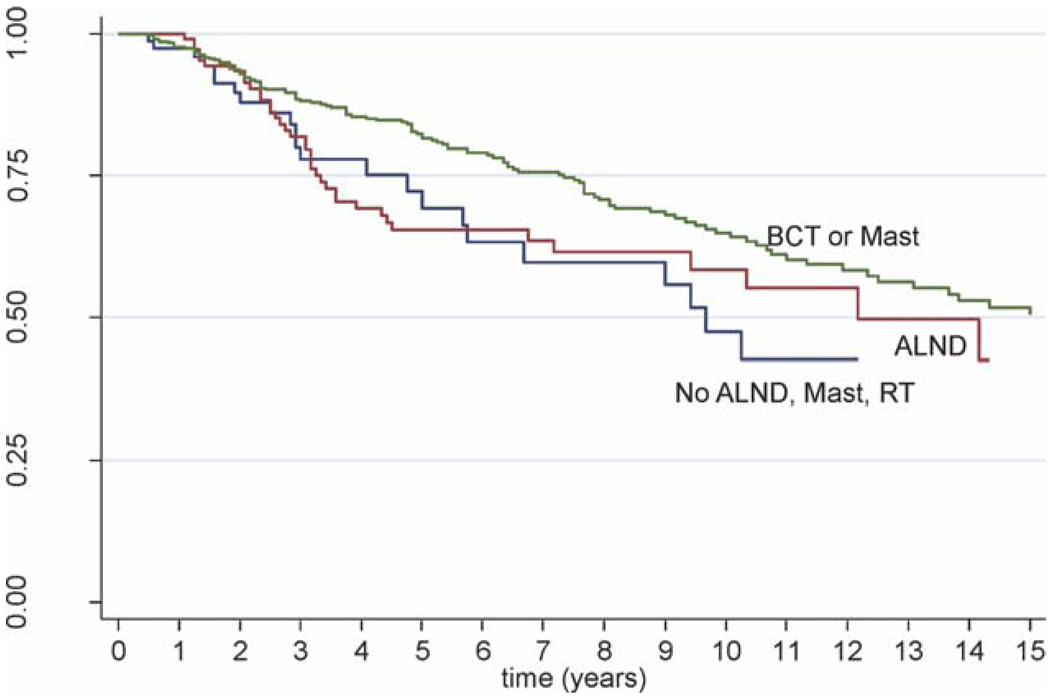
Methods: The cause-specific survival (CSS) and overall survival (OS) of women with T0N+M0 ductal, lobular, or mixed breast cancer in the Surveillance, Epidemiology, and End Results database from 1983 to 2006 were analyzed. Groups were defined as: 1) no ALND, mastectomy, or RT (observation); 2) ALND only; 3) mastectomy plus ALND with or without postmastectomy radiation (Mast); and 4) breast-conserving therapy (BCT) with ALND and radiation (BCT).
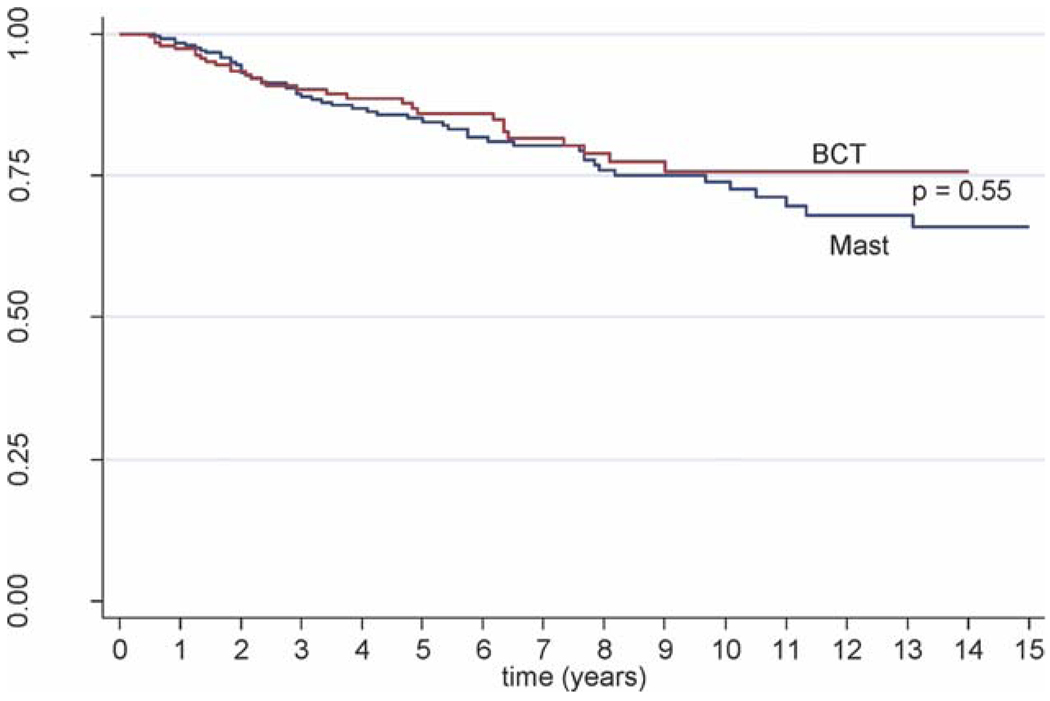
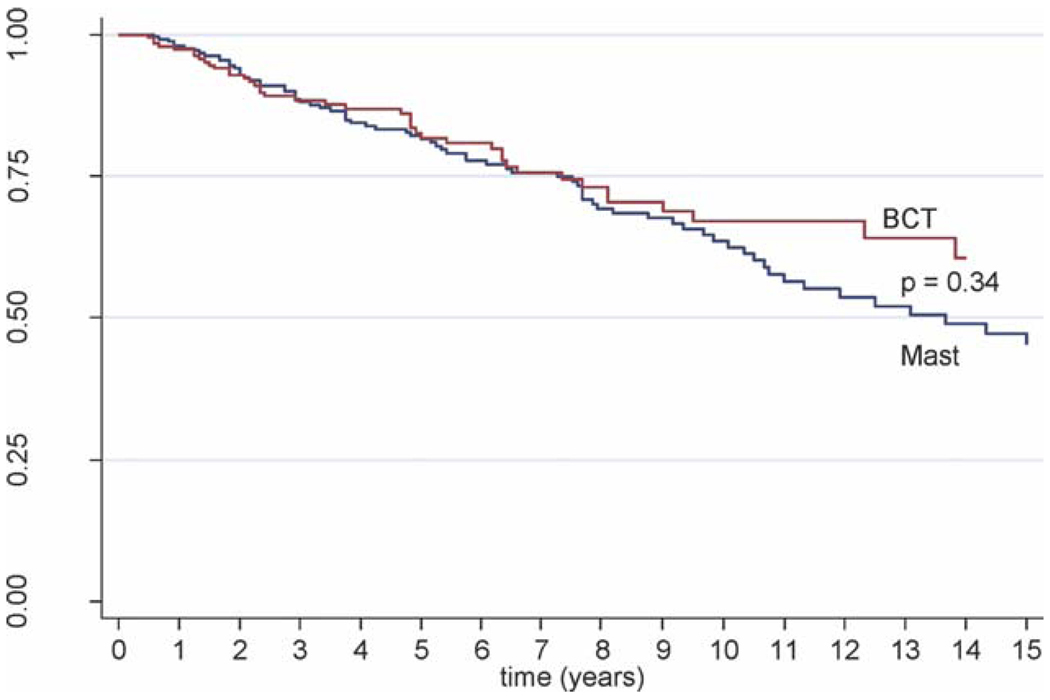
Results: In total, 750 of 770,030 patients with breast cancer had T0N+M0 disease (incidence, 0.10%), and 596 of those patients underwent ALND (79.5%). Patients who underwent Mast or BCT (n = 470) had a 10-year OS rate of 64.9% compared with 58.5% for patients who underwent ALND only (n = 126; P = .02) and 47.5% for patients who underwent observation only (n = 94; P = .04). The 10-year CSS rate was 75.7% for patients who underwent BCT versus 73.9% for patients who underwent Mast (P = .55). In multivariate analysis of CSS for patients who underwent Mast or BCT, the following factors were correlated with an unfavorable outcome: positive estrogen receptor status (hazard ratio [HR], 0.48; 95% confidence interval [CI], 0.24-0.96; P = .04), >/=10 positive lymph nodes (HR, 5.7; 95%CI, 2.4-13.4; P </= .01), and <10 resected lymph nodes (HR, 42.9; 95%CI, 1.2-7.1; P = .02). Mast did not improve CSS compared with BCT (HR, 1.09; 95%CI, 0.57-2.1; P = .79).
Conclusions: Definitive locoregional treatment with either Mast or BCT improved the outcome of patients with T0N+breast cancer, and no difference in survival was observed between the treatments. Cancer 2010. (c) 2010 American Cancer Society.
Conflict of interest statement
The authors made no disclosures.
Figures
References
-
- National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology, Breast Cancer v1.2009. [Accessed August 28, 2009]; Available at: http://www.nccn.org/professionals/physician_gls/PDF/breast.pdf.
-
- Vlastos G, Jean ME, Mirza AN, et al. Feasibility of breast preservation in the treatment of occult primary carcinoma presenting with axillary metastases. Ann Surg Oncol. 2001;8:425–431. - PubMed
-
- Foroudi F, Tiver KW. Occult breast carcinoma presenting as axillary metastases. Int J Radiat Oncol Biol Phys. 2000;47:143–147. - PubMed
-
- Shannon C, Walsh G, Sapunar F, A’Hern R, Smith I. Occult primary breast carcinoma presenting as axillary lymphadenopathy. Breast. 2002;11:414–418. - PubMed
-
- Zippin C, Lum D, Hankey BF. Completeness of hospital cancer case reporting from the SEER Program of the National Cancer Institute. Cancer. 1995;76:2343–2350. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
