

Abnormal microarchitecture and reduced stiffness at the radius and tibia in postmenopausal women with fractures
- PMID: 20564238
- PMCID: PMC3149820
- DOI: 10.1002/jbmr.152
Abnormal microarchitecture and reduced stiffness at the radius and tibia in postmenopausal women with fractures
Erratum in
- J Bone Miner Res. 2011 Feb;26(2):439
Abstract
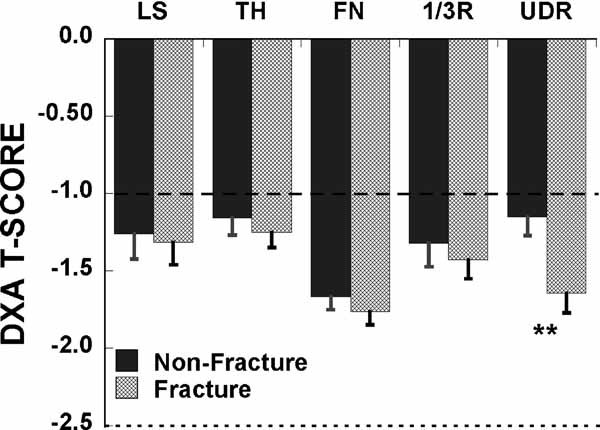
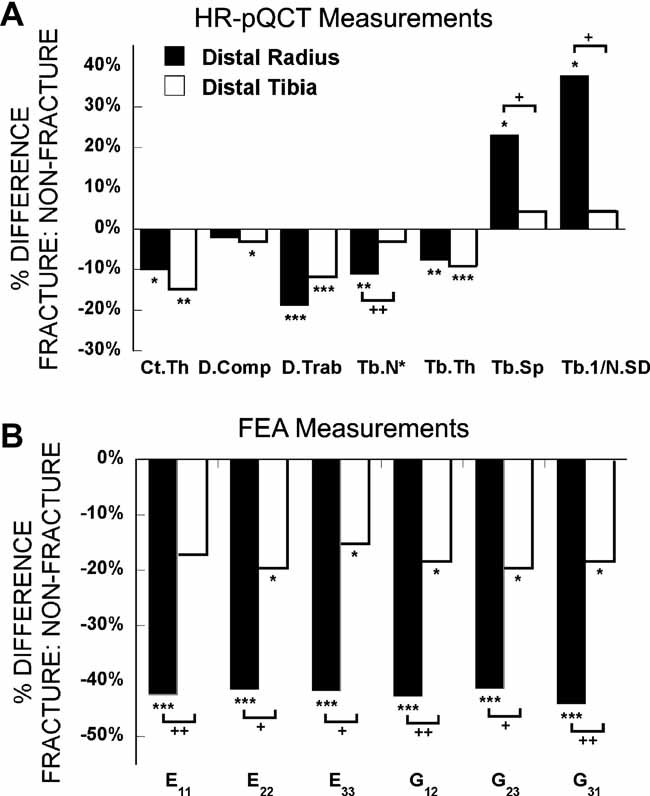
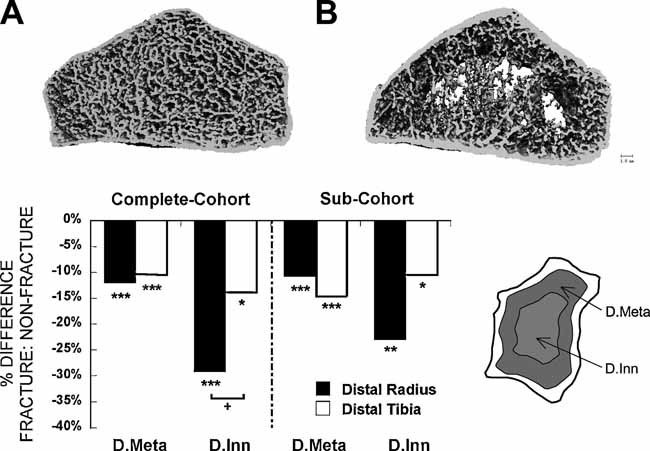
Measurement of areal bone mineral density (aBMD) by dual-energy x-ray absorptiometry (DXA) has been shown to predict fracture risk. High-resolution peripheral quantitative computed tomography (HR-pQCT) yields additional information about volumetric BMD (vBMD), microarchitecture, and strength that may increase understanding of fracture susceptibility. Women with (n = 68) and without (n = 101) a history of postmenopausal fragility fracture had aBMD measured by DXA and trabecular and cortical vBMD and trabecular microarchitecture of the radius and tibia measured by HR-pQCT. Finite-element analysis (FEA) of HR-pQCT scans was performed to estimate bone stiffness. DXA T-scores were similar in women with and without fracture at the spine, hip, and one-third radius but lower in patients with fracture at the ultradistal radius (p < .01). At the radius fracture, patients had lower total density, cortical thickness, trabecular density, number, thickness, higher trabecular separation and network heterogeneity (p < .0001 to .04). At the tibia, total, cortical, and trabecular density and cortical and trabecular thickness were lower in fracture patients (p < .0001 to .03). The differences between groups were greater at the radius than at the tibia for inner trabecular density, number, trabecular separation, and network heterogeneity (p < .01 to .05). Stiffness was reduced in fracture patients, more markedly at the radius (41% to 44%) than at the tibia (15% to 20%). Women with fractures had reduced vBMD, microarchitectural deterioration, and decreased strength. These differences were more prominent at the radius than at the tibia. HR-pQCT and FEA measurements of peripheral sites are associated with fracture prevalence and may increase understanding of the role of microarchitectural deterioration in fracture susceptibility. © 2010 American Society for Bone and Mineral Research.
Copyright © 2010 American Society for Bone and Mineral Research.
Figures
References
-
- National Osteoporosis Foundation. America's Bone Health: The State of Osteoporosis and Low Bone Mass in Our Nation. Washington: National Osteoporosis Foundation; 2002. pp. 1–55.
-
- Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporos Int. 1997;7:407–413. - PubMed
-
- Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res. 2007;22:465–475. - PubMed
-
- Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359:1761–1767. - PubMed
-
- Hannan EL, Magaziner J, Wang JJ, et al. Mortality and locomotion 6 months after hospitalization for hip fracture: risk factors and risk-adjusted hospital outcomes. JAMA. 2001;285:2736–2742. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
