

Simulated reflux decreases vocal fold epithelial barrier resistance
- PMID: 20564752
- PMCID: PMC2927501
- DOI: 10.1002/lary.20983
Simulated reflux decreases vocal fold epithelial barrier resistance
Abstract
Objectives/hypothesis: The vocal fold epithelium provides a barrier to the entry of inhaled and systemic challenges. However, the location of the epithelium makes it vulnerable to damage. Past research suggests, but does not directly demonstrate, that exposure to gastric reflux adversely affects the function of the epithelial barrier. Understanding the nature of reflux-induced epithelial barrier dysfunction is necessary to better recognize the mechanisms for vocal fold susceptibility to this disease. Therefore, we examined the effects of physiologically relevant reflux challenges on vocal fold transepithelial resistance and gross epithelial and subepithelial appearance.
Study design: Ex vivo, mixed design with between-group and repeated-measures analyses.
Methods: Healthy, native porcine vocal folds (N = 52) were exposed to physiologically relevant acidic pepsin, acid-only, or pepsin-only challenges and examined with electrophysiology and light microscopy. For all challenges, vocal folds exposed to a neutral pH served as control.
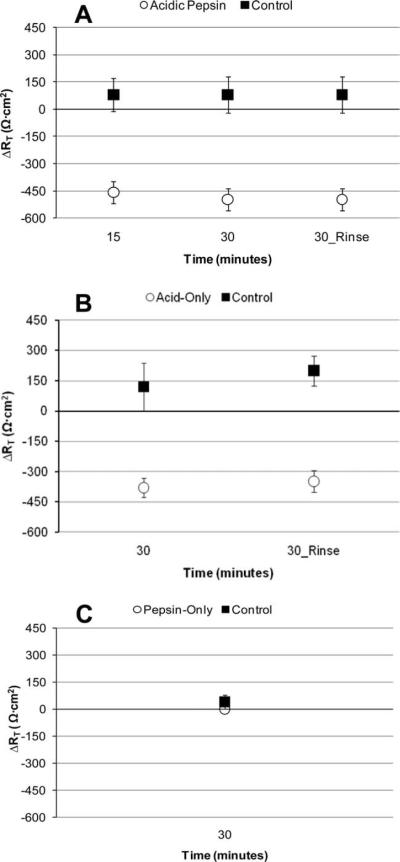
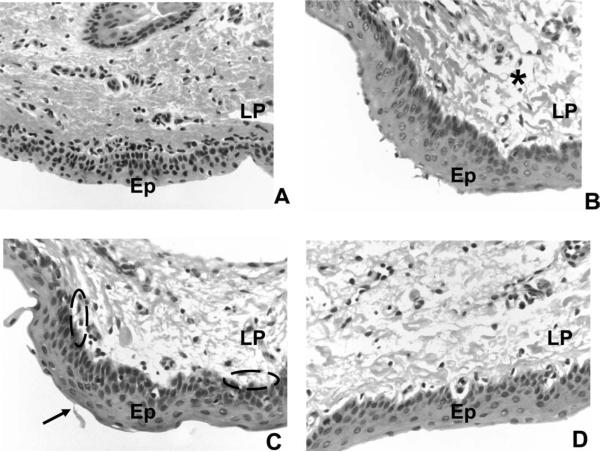
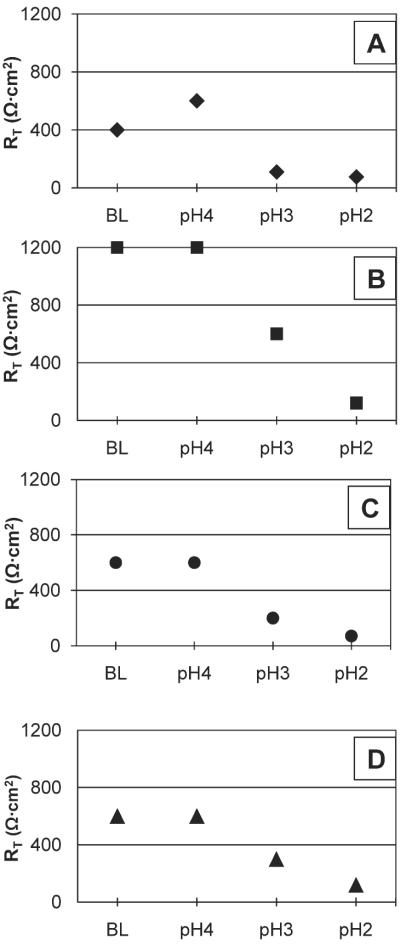
Results: Acidic pepsin and acid-only challenges, but not pepsin-only or control challenges significantly reduced transepithelial resistance within 30 minutes. Reductions in transepithelial resistance were irreversible. Challenge exposure produced minimal gross changes in vocal fold epithelial or subepithelial appearance as evidenced by light microscopy.
Conclusions: These findings demonstrate that acidic environments characteristic of gastric reflux compromise epithelial barrier function without gross structural changes. In healthy, native vocal folds, reductions in transepithelial resistance could reflect reflux-related epithelial disruption. These results might guide the development of pharmacologic and therapeutic recommendations for patients with reflux, such as continued acid-suppression therapy and patient antireflux behavioral education.
Figures
References
-
- Rees C, Belfasky P. Laryngopharyngeal reflux: current concepts in pathophysiology, diagnosis, and treatment. Int J of Speech Lang Pathol. 2008;10:245–253. - PubMed
-
- Connor N, Palazzi-Churas K, Cohen S, Leverson G, Bless D. Symptoms of extraesophageal reflux in a community-dwelling sample. J Voice. 2007;12:189–202. - PubMed
-
- Koufman JA. The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope. 1991;101(4 pt 2suppl 53):1–78. - PubMed
-
- Johnston N, Bulmer D, Gill GA, et al. Cell biology of laryngeal epithelial defenses in health and disease: further studies. Ann Otol Rhinol Laryngol. 2003;112:481–491. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
