

Accuracy of general practitioners' assessment of chest pain patients for coronary heart disease in primary care: cross-sectional study with follow-up
- PMID: 20564768
- PMCID: PMC2897083
- DOI: 10.3325//cmj.2010.51.243
Accuracy of general practitioners' assessment of chest pain patients for coronary heart disease in primary care: cross-sectional study with follow-up
Abstract
Aim: To estimate how accurately general practitioners' (GP) assessed the probability of coronary heart disease in patients presenting with chest pain and analyze the patient management decisions taken as a result.
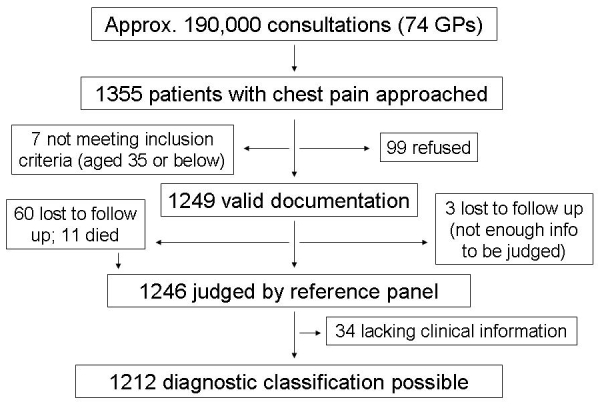
Methods: During 2005 and 2006, the cross-sectional diagnostic study with a delayed-type reference standard included 74 GPs in the German state of Hesse, who enrolled 1249 consecutive patients presenting with chest pain. GPs recorded symptoms and findings for each patient on a report form. Patients and GPs were contacted 6 weeks and 6 months after the patients' visit to the GP. Data on chest complaints, investigations, hospitalization, and medication were reviewed by an independent panel, with coronary heart disease being the reference condition. Diagnostic properties (sensitivity, specificity, and predictive values) of the GPs' diagnoses were calculated.
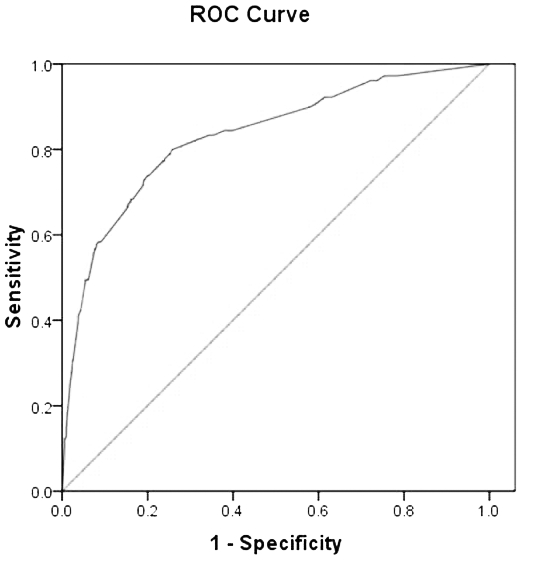
Results: GPs diagnosed coronary heart disease with the sensitivity of 69% (95% confidence interval [CI], 62-75) and specificity of 89% (95% CI, 87-91), and acute coronary syndrome with the sensitivity of 50% (95% CI, 36-64) and specificity of 98% (95% CI, 97-99). They assumed coronary heart disease in 245 patients, 41 (17%) of whom were referred to the hospital, 77 (31%) to a cardiologist, and 162 (66%) to electrocardiogram testing.
Conclusions: GPs' evaluation of chest pain patients, based on symptoms and signs alone, was not sufficiently accurate for diagnosing or excluding coronary heart disease or acute coronary syndrome.
Figures
References
-
- Klinkman MS, Stevens D, Gorenflo DW. Episodes of care for chest pain: a preliminary report from MIRNET. Michigan Research Network. J Fam Pract. 1994;38:345–52. - PubMed
-
- Verdon F, Herzig L, Burnand B, Bischoff T, Pecoud A, Junod M, et al. Chest pain in daily practice: occurrence, causes and management. Swiss Med Wkly. 2008;138:340–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical