

Feasibility of neuromuscular training in patients with severe hip or knee OA: the individualized goal-based NEMEX-TJR training program
- PMID: 20565735
- PMCID: PMC2896351
- DOI: 10.1186/1471-2474-11-126
Feasibility of neuromuscular training in patients with severe hip or knee OA: the individualized goal-based NEMEX-TJR training program
Abstract
Background: Although improvements are achieved by general exercise, training to improve sensorimotor control may be needed for people with osteoarthritis (OA). The aim was to apply the principles of neuromuscular training, which have been successfully used in younger and middle-aged patients with knee injuries, to older patients with severe hip or knee OA. We hypothesized that the training program was feasible, determined as: 1) at most acceptable self-reported pain following training; 2) decreased or unchanged pain during the training period; 3) few joint specific adverse events related to training, and 4) achieved progression of training level during the training period.
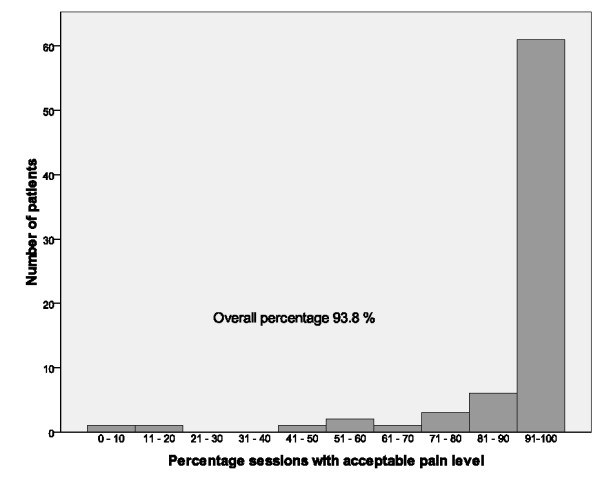
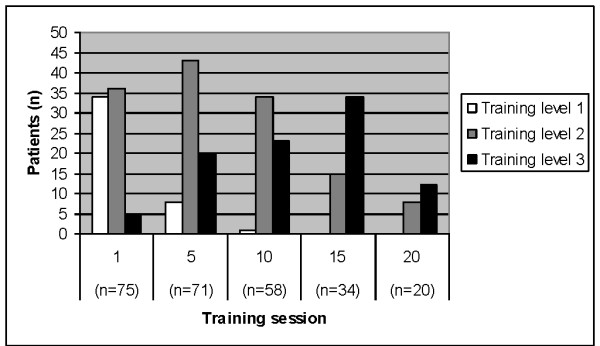
Methods: Seventy-six patients, between 60 and 77 years, with severe hip (n = 38, 55% women) or knee OA (n = 38, 61% women) underwent an individualized, goal-based neuromuscular training program (NEMEX-TJR) in groups for a median of 11 weeks (quartiles 7 to 15) prior to total joint replacement (TJR). Pain was self-reported immediately after each training session on a 0 to 10 cm, no pain to pain as bad as it could be, scale, where 0-2 indicates safe, > 2 to 5 acceptable and > 5 high risk pain. Joint specific adverse events were: not attending or ceasing training because of increased pain/problems in the index joint related to training, and self-reported pain > 5 after training. The level of difficulty of training was registered.
Results: Patients with severe OA of the hip or knee reported safe pain (median 2 cm) after training. Self-reported pain was lower at training sessions 10 and 20 (p = 0.04) and unchanged at training sessions 5 and 15 (p = 0.170, p = 0.161) compared with training session 1. There were no joint specific adverse events in terms of not attending or ceasing training. Few patients (n = 17, 22%) reported adverse events in terms of self-reported pain > 5 after one or more training sessions. Progression of training level was achieved over time (p < 0.001).
Conclusions: The NEMEX-TJR training program is feasible in patients with severe hip or knee OA, in terms of safe self-reported pain following training, decreased or unchanged pain during the training period, few joint specific adverse events, and achieved progression of training level during the training period.
Figures
References
-
- Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, Bierma-Zeinstra S, Brandt KD, Croft P, Doherty M. et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. 2008;11(2):137–162. doi: 10.1016/j.joca.2007.12.013. - DOI - PubMed
-
- Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, Bierma-Zeinstra S, Brandt KD, Croft P, Doherty M. et al. OARSI recommendations for the management of hip and knee osteoarthritis, part I: critical appraisal of existing treatment guidelines and systematic review of current research evidence. Osteoarthritis Cartilage. 2007;11(9):981–1000. doi: 10.1016/j.joca.2007.06.014. - DOI - PubMed
-
- Fransen M, McConnell S. Exercise for osteoarthritis of the knee. Cochrane Database Syst Rev. 2008. p. CD004376. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
