

Association between adherence to calcium-channel blocker and statin medications and likelihood of cardiovascular events among US managed care enrollees
- PMID: 20565779
- PMCID: PMC2897772
- DOI: 10.1186/1471-2261-10-29
Association between adherence to calcium-channel blocker and statin medications and likelihood of cardiovascular events among US managed care enrollees
Abstract
Background: Prior studies have found that patients taking single-pill amlodipine/atorvastatin (SPAA) have greater likelihood of adherence at 6 months than those taking 2-pill calcium-channel blocker and statin combinations (CCB/statin). This study examines whether this adherence benefit results in fewer cardiovascular (CV) events.
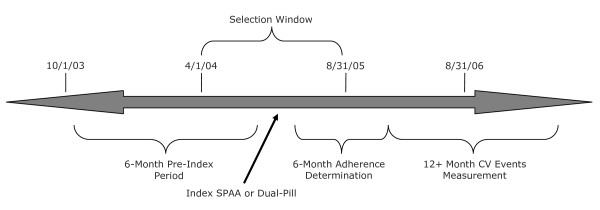
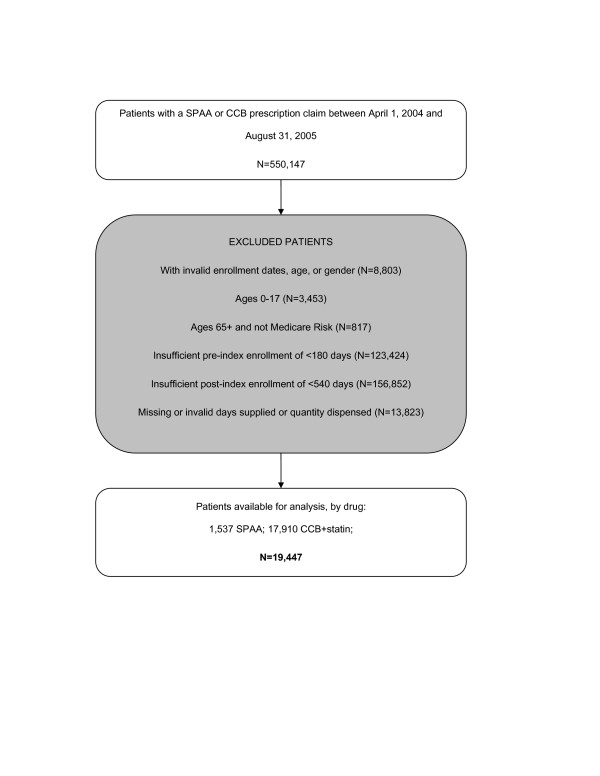
Methods: A retrospective cohort study was conducted using administrative claims data from the IMS LifeLink: US Health Plan Claims database, identifying adults already taking CCB or statin (but not both) who had an index event of either initiating treatment with SPAA or adding CCB to statin (or vice versa) between April 1, 2004 to August 31, 2005. Inclusion criteria included age 18+ years, continuously enrolled for minimum of 6 months prior and 18 months following treatment initiation, >1 diagnosis of hypertension, and no prescription claims for SPAA or added CCB or statin for 6 months prior. Exclusion criteria included >1 claim with missing or invalid days supplied, age 65+ years and not enrolled in Medicare Advantage, or history of prior CV events, cancer diagnosis, or chronic renal failure. The primary outcome measure was the rate of CV events (myocardial infarction, heart failure, angina, other ischemic heart disease, stroke, peripheral vascular disease, or revascularization procedure) from 6 to 18 months following index date, analyzed at three levels: 1) all adherent vs. non-adherent patients, 2) SPAA vs. dual-pill patients (regardless of adherence level), and 3) adherent SPAA, adherent dual-pill, and non-adherent SPAA patients vs. non-adherent dual-pill patients.
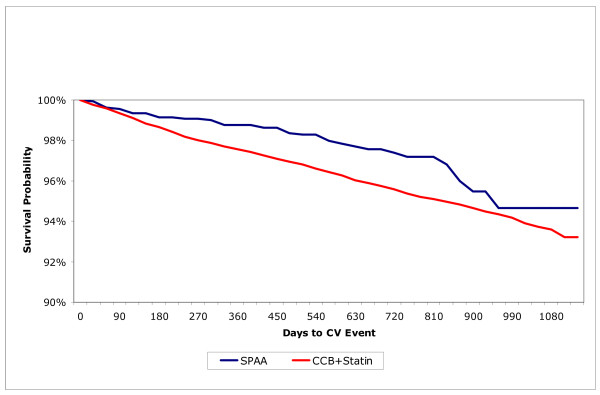
Results: Of 1,537 SPAA patients, 56.5% were adherent at 6 months, compared with 21.4% of the 17,910 CCB/statin patients (p < 0.001). Logistic regression found SPAA patients more likely to be adherent (OR = 4.7, p < 0.001) than CCB/statin patients. In Cox proportional hazards models, being adherent to either regimen was associated with significantly lower risk of CV event (HR = 0.77, p = 0.003). A similar effect was seen for SPAA vs. CCB/statin patients (HR = 0.68, p = 0.02). In a combined model, the risk of CV events was significantly lower for adherent CCB/statin patients (HR = 0.79, p = 0.01) and adherent SPAA patients (HR = 0.61, p = 0.03) compared to non-adherent CCB/statin patients.
Conclusions: Patients receiving SPAA rather than a 2-pill CCB/statin regimen are more likely to be adherent. In turn, adherence to CCB and statin medications is associated with lower risk of CV events in primary prevention patients.
Figures
Similar articles
-
Does a single-pill antihypertensive/lipid-lowering regimen improve adherence in US managed care enrolees? A non-randomized, observational, retrospective study.Am J Cardiovasc Drugs. 2010;10(3):193-202. doi: 10.2165/11530680-000000000-00000. Am J Cardiovasc Drugs. 2010. PMID: 20387911
-
Adherence with single-pill amlodipine/atorvastatin vs a two-pill regimen.Vasc Health Risk Manag. 2008;4(3):673-81. Vasc Health Risk Manag. 2008. PMID: 18827917 Free PMC article.
-
Cardiovascular outcomes among patients newly initiating atorvastatin or simvastatin therapy: a large database analysis of managed care plans in the United States.Clin Ther. 2008 Jan;30(1):195-205. doi: 10.1016/j.clinthera.2008.01.003. Clin Ther. 2008. PMID: 18343257
-
A single-pill combination of amlodipine besylate and atorvastatin calcium.Drugs Today (Barc). 2006 Mar;42(3):157-75. doi: 10.1358/dot.2006.42.3.953593. Drugs Today (Barc). 2006. PMID: 16628258 Review.
-
Atorvastatin calcium plus amlodipine for the treatment of hypertension.Expert Opin Pharmacother. 2012 Dec;13(18):2673-85. doi: 10.1517/14656566.2012.742064. Epub 2012 Nov 10. Expert Opin Pharmacother. 2012. PMID: 23140185 Review.
Cited by
-
Combining antihypertensive and antihyperlipidemic agents - optimizing cardiovascular risk factor management.Integr Blood Press Control. 2011;4:55-71. doi: 10.2147/IBPC.S12215. Epub 2011 Nov 15. Integr Blood Press Control. 2011. PMID: 22162939 Free PMC article.
-
Adherence to statins and its impact on clinical outcomes: a retrospective population-based study in China.BMC Cardiovasc Disord. 2020 Jun 10;20(1):282. doi: 10.1186/s12872-020-01566-2. BMC Cardiovasc Disord. 2020. PMID: 32522146 Free PMC article.
-
Cost-effectiveness analysis of low density lipoprotein cholesterol-lowering therapy in hypertensive patients with type 2 diabetes in Korea: single-pill regimen (amlodipine/atorvastatin) versus double-pill regimen (amlodipine+atorvastatin).Epidemiol Health. 2015 Feb 22;37:e2015010. doi: 10.4178/epih/e2015010. Epidemiol Health. 2015. PMID: 25773438 Free PMC article.
-
Amlodipine + atorvastatin single pill is the most effective choice for primary prevention.Cardiovasc J Afr. 2010 Jul-Aug;21(4):243. Cardiovasc J Afr. 2010. PMID: 20838732 Free PMC article. No abstract available.
-
Nonadherence to Cardiovascular Drugs Predicts Risk for Non-Arthritic Anterior Ischemic Optic Neuropathy: A Large-Scale National Study.J Clin Med. 2024 Aug 9;13(16):4670. doi: 10.3390/jcm13164670. J Clin Med. 2024. PMID: 39200811 Free PMC article.
References
-
- World Health Organization. Cardiovascular diseases (CVDs). Fact sheet number 317. Updated September 2009. http://www.who.int/mediacentre/factsheets/fs317/en/index.html
-
- Neaton JD, Wentworth D. Serum cholesterol, blood pressure, cigarette smoking, and death from coronary heart disease. Overall findings and differences by age for 316,099 white men. Multiple Risk Factor Intervention Trial Research Group. Arch Intern Med. 1992;152:56–64. doi: 10.1001/archinte.152.1.56. - DOI - PubMed
-
- ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) JAMA. 2002;288:2981–2997. doi: 10.1001/jama.288.23.2981. - DOI - PubMed
-
- Sever P, Dahlöf B, Poulter N, Wedel H, Beevers G, Caulfield M, Collins R, Kjeldsen S, Kristinsson A, McInnes G. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet. 2003;361:1149–1158. doi: 10.1016/S0140-6736(03)12948-0. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
