

A systematic review of population based epidemiological studies in Myasthenia Gravis
- PMID: 20565885
- PMCID: PMC2905354
- DOI: 10.1186/1471-2377-10-46
A systematic review of population based epidemiological studies in Myasthenia Gravis
Abstract
Background: The aim was to collate all myasthenia gravis (MG) epidemiological studies including AChR MG and MuSK MG specific studies. To synthesize data on incidence rate (IR), prevalence rate (PR) and mortality rate (MR) of the condition and investigate the influence of environmental and technical factors on any trends or variation observed.
Methods: Studies were identified using multiple sources and meta-analysis performed to calculate pooled estimates for IR, PR and MR.
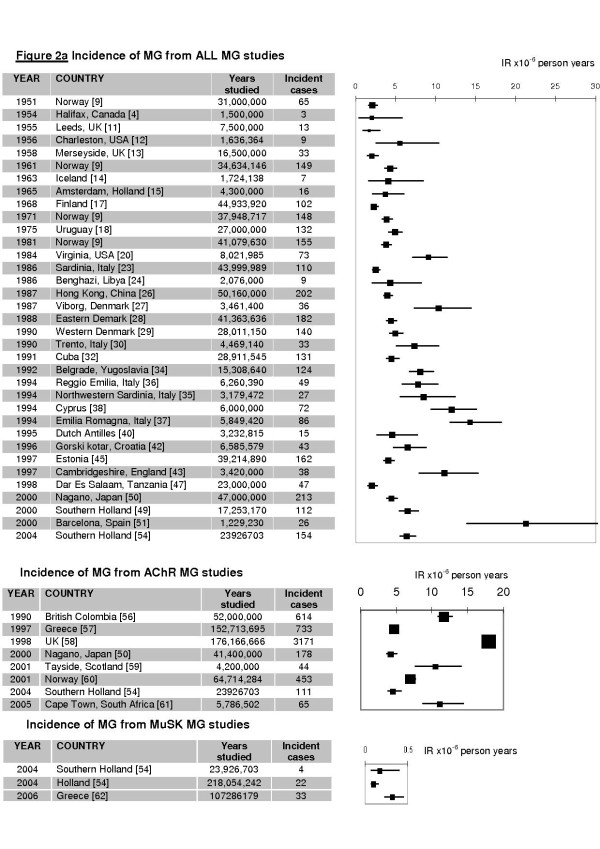
Results: 55 studies performed between 1950 and 2007 were included, representing 1.7 billion population-years. For All MG estimated pooled IR (eIR): 5.3 per million person-years (C.I.:4.4, 6.1), range: 1.7 to 21.3; estimated pooled PR: 77.7 per million persons (C.I.:64.0, 94.3), range 15 to 179; MR range 0.1 to 0.9 per millions person-years. AChR MG eIR: 7.3 (C.I.:5.5, 7.8), range: 4.3 to 18.0; MuSK MG IR range: 0.1 to 0.32. However marked variation persisted between populations studied with similar methodology and in similar areas.
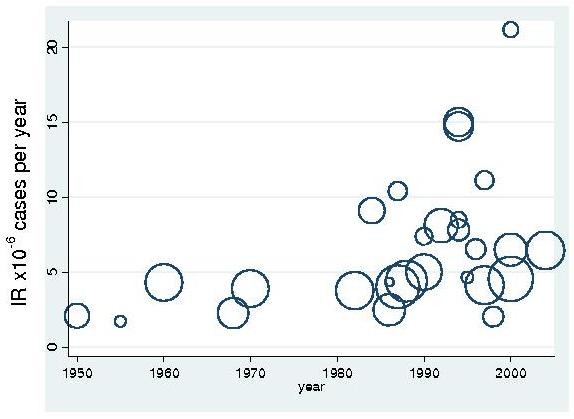
Conclusions: We report marked variation in observed frequencies of MG. We show evidence of increasing frequency of MG with year of study and improved study quality. This probably reflects improved case ascertainment. But other factors must also influence disease onset resulting in the observed variation in IR across geographically and genetically similar populations.
Figures

References
-
- Lindstrom JM, Seybold ME, Lennon VA. Antibody to acetylcholine receptor in myasthenia gravis. Prevalence, clinical correlates, and diagnostic value. Neurology. 1976;26(11):1054–9. - PubMed
-
- Kurtzke JF. Epidemiology of myasthenia gravis. Advances in Neurology. 1978;19:545–566. - PubMed
-
- Phillips LH, Torner JC. Epidemiologic evidence for changing natural history of myasthenia gravis. Neurology. 1996;47:1233–1238. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
