

doi: 10.1177/159101990701300402.
Epub 2008 Feb 1.
Extracranial vertebral artery involvement in neurofibromatosis type I. Report of four cases and literature review
Affiliations
- PMID: 20566100
- PMCID: PMC3329237
- DOI: 10.1177/159101990701300402
Item in Clipboard
Extracranial vertebral artery involvement in neurofibromatosis type I. Report of four cases and literature review
Interv Neuroradiol.
2007 Dec.
Abstract
Neurofibromatosis type 1 (NF-1) is one of the most common inherited diseases and as an autosomal dominant genetic disorder results from NF-1 gene mutation with 100% penetration and wide phenotypic variability. The disease can involve a wide variety of tissues derived from all three embryonic layers. NF-1 vasculopathy has been described primarily in peripheral arteries, but arteries supplying the CNS may also be involved. Of those, extracranial vertebral involvement is the commonest and most important. A series of four patients with NF-1 and vascular disease of the vertebral artery is described with a review of the pathophysiology, vascular phenotypes, their management and the pertinent literature.
Figures
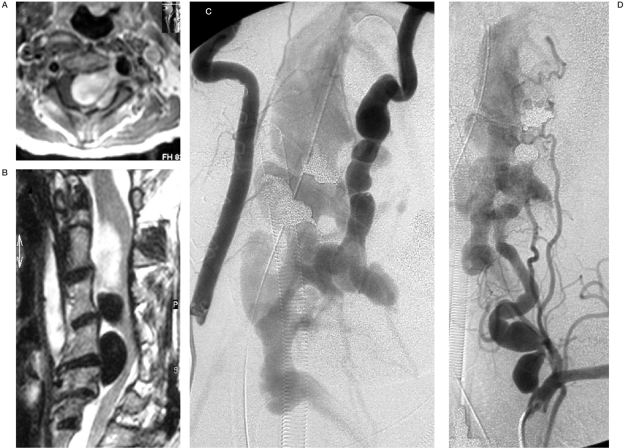
Case 1. A) Sagittal T2-W MRI (A) revealing large flow void epidural structures at C2-5, compatible with venous pouches and a partially thrombosed superior portion, causing severe cord compression. B) Axial T1-W MRI post Gd enhancement showing extension of the epidural venous pouches along the left neural foramen with nerve root compressions. C,D) Right and left vertebral angiograms demonstrating AV shunting from the LVA at C4 level, compatible with VVAVF. Dysplastic change and tortuousity of the LVA proximal and distal to the fistula are also noted with indirect collaterals from the left ascending cervical artery and thyrocervical trunk due to a "sump effect".
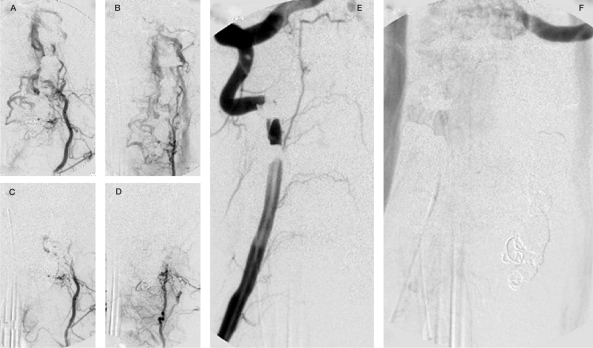
Case 1 (continued),A,B) Left cervical arteries angiogram: collateral contribution to the fistula throughout deep cervical and thyrocervical trunk. C,D) The control after glue and particle embolization. E,F) The right vertebral angiographic control after completed left vertebral occlusion with no remaining fistula.
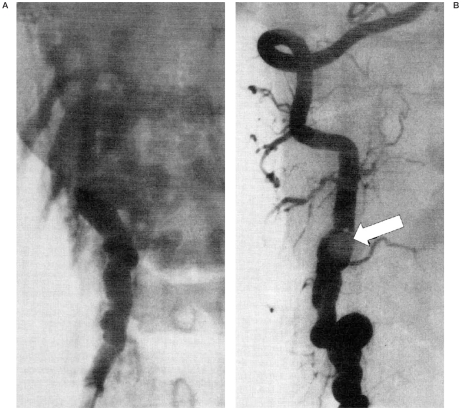
Case 2. Right vertebral angiogram AP view pre and post gold valve balloon (GVB) embolization demonstrating dysplastic change of the RVA with early filling of the epidural venous plexus at C4 level which completely disappeared after deployment of one No. 9 GVB that enabled preservation of the RVA.
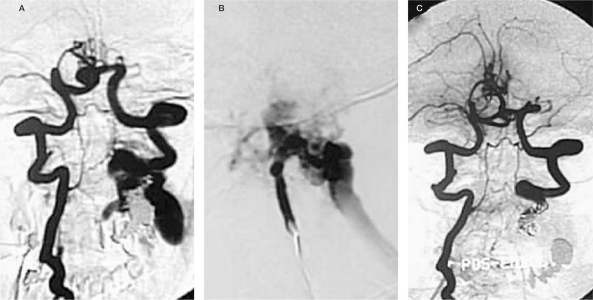
Case 3. Right vertebral angiogram, AP view, pre-embolization (A) and left vertebral angiogram (B) lateral view pre-embolization both demonstrate an AV shunt at the left C3-4 level, with venous blood draining into dilated epidural pouches and then further draining into the jugular veins. There is complete obliteration of the VVAVF after GDC embolization and sacrifice of the LVA (C, right VA angiogram, AP view).
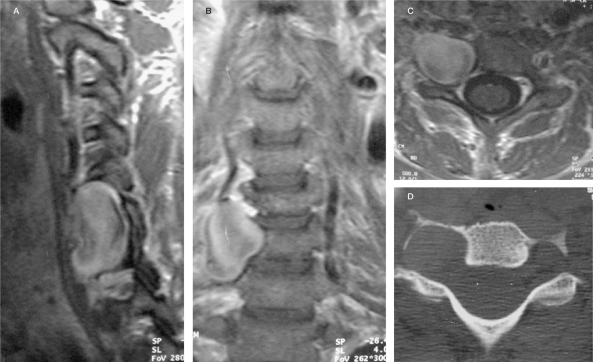
Case 4. On T2W MRI sequences enlargement of transverse foramen due to a mass presumably representing a large aneurysm (high signal due to low flow and turbulence) can be seen that demonstrates contrast enhancement (A-C: T1 weighted images after contrast) and bone erosion on CT (D). Adjacent structures are compressed.
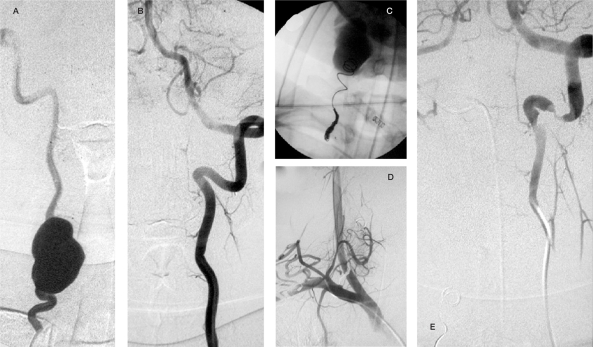
Case 4 . Angiography (A: right vertebral artery injection, B: left vertebral artery injection) reveals a large fusiform shaped aneurysm at C5-6 level of the RVA with good supply to the posterior circulation through the LVA. After GDC embolization contrast stagnation in the aneurysm was noted immediately after sacrifice of the proximal RVA. Post embolization angiograms (D,E) confirmed complete obliteration of the aneurysm.
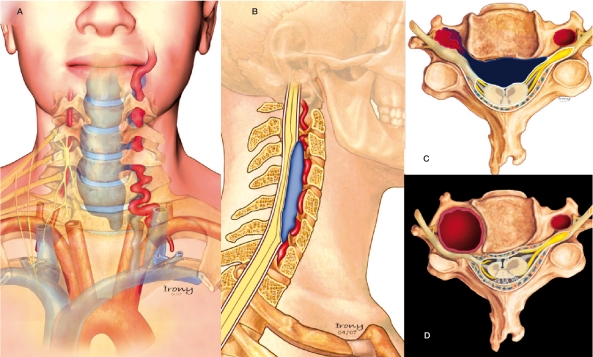
Schematic Illustration of the pathophysiology of the presented cases. In the first three patients, a vertebrovertebral arteriovenous fistula was present. In these drawings, the dysplastic artery ruptured to a venous vertebral compartment and major important reflux to the epidural venous plexus causing spinal cord and radicular compression can be appreciated (AC). D) Illustration of the vertebral aneurysm with irregular and thick walls of the RVA associated with adjacent bone erosion from the pulsatility and enlargement of the transverse foramen causing compression of the exiting nerve root as was present in patient 4.
Similar articles
-
[Neurofibromatosis associated with intra- and extracranial aneurysms and extracranial vertebral arteriovenous fistula].No Shinkei Geka. 1985 Aug;13(8):875-80. No Shinkei Geka. 1985. PMID: 3932894 Japanese.
-
Cervical vertebral artery aneurysms and arteriovenous fistulae in neurofibromatosis type 1: case reports.Neurosurgery. 1991 Nov;29(5):760-5. doi: 10.1097/00006123-199111000-00020. Neurosurgery. 1991. PMID: 1961409
-
Extracranial vertebral artery aneurysm ruptured into the thoracic cavity with neurofibromatosis type 1: case report.Neurosurgery. 2004 Jun;54(6):1517-20; discussion 1520-1. doi: 10.1227/01.neu.0000125547.31328.69. Neurosurgery. 2004. PMID: 15157311
-
Neurofibromatosis Type 1-Associated Extracranial Vertebral Artery Aneurysm Complicated by Vertebral Arteriovenous Fistula After Rupture: Case Report and Literature Review.World Neurosurg. 2016 Dec;96:609.e13-609.e18. doi: 10.1016/j.wneu.2016.09.036. Epub 2016 Sep 16. World Neurosurg. 2016. PMID: 27647034 Review.
-
Subarachnoid hemorrhage in neurofibromatosis type 1: case report of extracranial cerebral aneurysm rupture into a meningocele.J Neuroradiol. 2011 May;38(2):125-8. doi: 10.1016/j.neurad.2010.11.001. Epub 2011 Jan 6. J Neuroradiol. 2011. PMID: 21215453 Review.
Cited by
-
Endovascular Embolization of a Dissected External Carotid Artery Pseudoaneurysm in a Young Female with Neurofibromatosis Complicated by Preeclampsia.Case Rep Vasc Med. 2019 Jun 12;2019:6020393. doi: 10.1155/2019/6020393. eCollection 2019. Case Rep Vasc Med. 2019. PMID: 31285934 Free PMC article.
-
Transcatheter arterial embolization for shock caused by intratumoral hemorrhaging in neurofibromatosis type 1: a report of two cases.Case Rep Dermatol. 2014 Feb 20;6(1):59-65. doi: 10.1159/000360216. eCollection 2014 Jan. Case Rep Dermatol. 2014. PMID: 24707252 Free PMC article.
-
Spontaneous obliteration of spontaneous vertebral arteriovenous fistula associated with fibromuscular dysplasia after partial surgery: A case report.Interv Neuroradiol. 2016 Dec;22(6):717-727. doi: 10.1177/1591019916659263. Epub 2016 Aug 1. Interv Neuroradiol. 2016. PMID: 27481913 Free PMC article.
-
[Neurovascular pathology in a patient with neurofibromatosis type 1. Case report].Rev Neurol. 2024 Aug 16;79(4):115-118. doi: 10.33588/rn.7904.2024172. Rev Neurol. 2024. PMID: 39078031 Free PMC article. Spanish.
-
Parachordal fistula--a case report and a short review.Neuroradiol J. 2016 Feb;29(1):82-5. doi: 10.1177/1971400915595578. Epub 2016 Jan 29. Neuroradiol J. 2016. PMID: 26825132 Free PMC article. Review.
References
-
- Riccardi VM. Neurofibromatosis update. Neurofibromatosis. 1989;2(5-6):284–291. - PubMed
-
- Riccardi VM. Neurofibromatosis. Neurol Clin. 1987;5(3):337–349. - PubMed
-
- Jentarra G, Snyder SL, Narayanan V. Genetic aspects of neurocutaneous disorders. Semin Pediatr Neurol. 2006;13(1):43–47. - PubMed
-
- Riccardi VM. Neurofibromatosis: Phenotype, Natural History and Pathogenesis. 2nd ed. Baltimore, MD: Johns Hopkins University Press; 1992.
-
- Fujimura T, et al. Neurofibromatosis 1 associated with an intracranial artery abnormality, moyamoya disease and bilateral congenital large hairy pigmented macules. Br J Dermatol. 2004;150(3):611–613. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
