

Unruptured Intracranial Aneurysms. Opinions of Experts in Endovascular Treatment Are Coherent,Weighted in Favour of Treatment, and Incompatible with ISUIA
- PMID: 20566114
- PMCID: PMC3345486
- DOI: 10.1177/159101990701300302
Unruptured Intracranial Aneurysms. Opinions of Experts in Endovascular Treatment Are Coherent,Weighted in Favour of Treatment, and Incompatible with ISUIA
Abstract
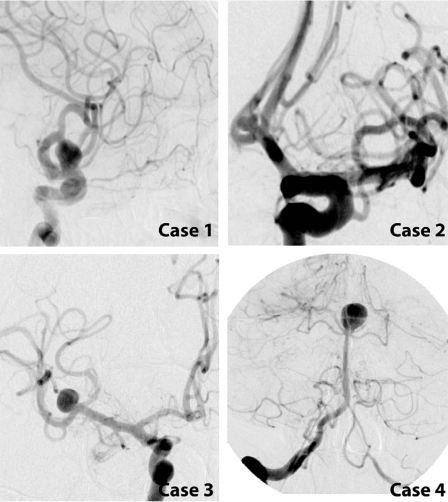
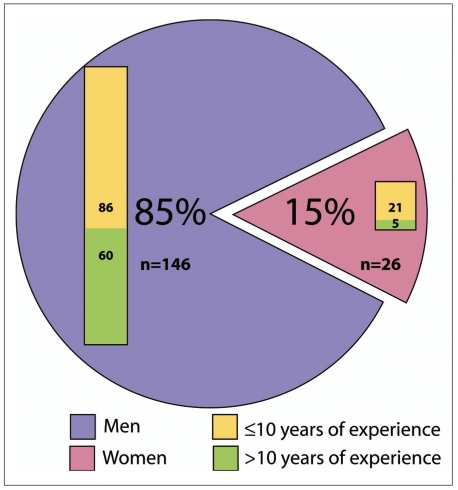
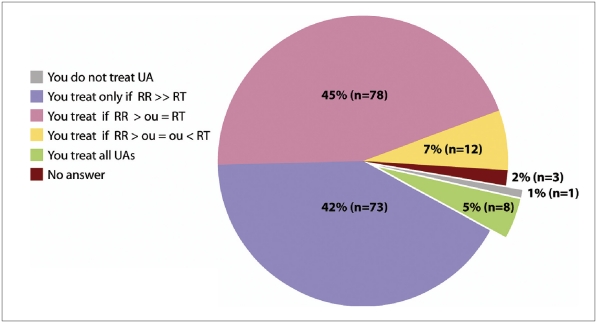
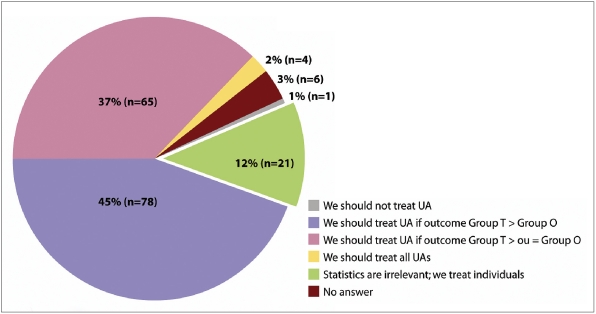
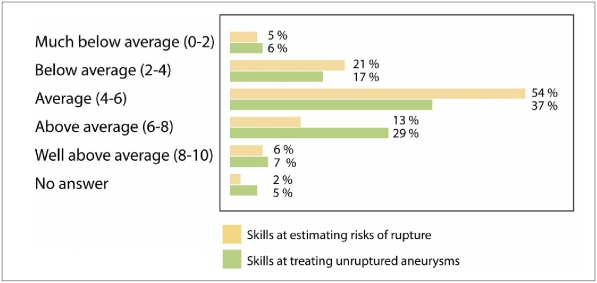
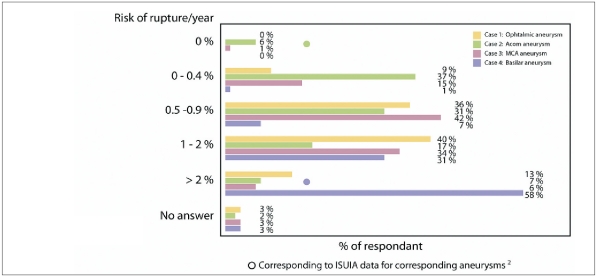
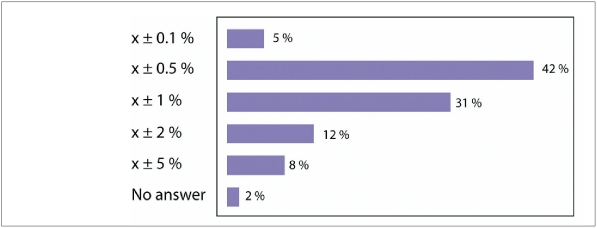
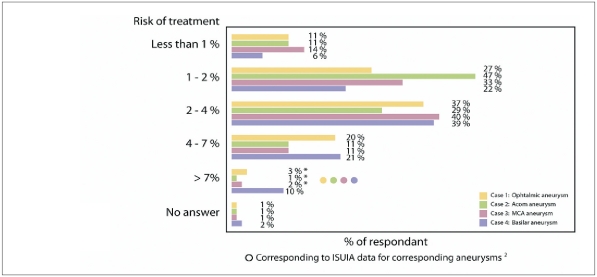
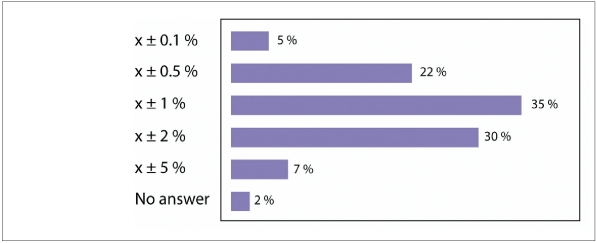
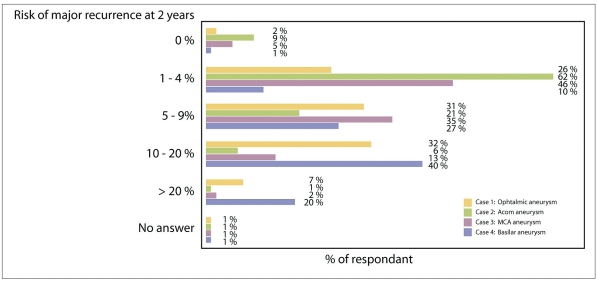
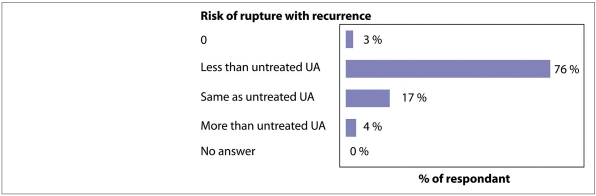
In the absence of level one evidence, the treatment of unruptured intracranial aneurysms is grounded on opinions. Results of the largest registry available, ISUIA (the International Study on Unruptured Intraacranial Aneurysms) suggest that surgical or endovascular treatments are rarely justified. Yet the unruptured aneurysm is the most frequent indication for treatment in many endovascular centres. In preparation for the initiation of a randomized trial, we aimed at a better knowledge of endovascular expert opinions on unruptured aneurysms. We administered a standard questionnaire to 175 endovascular experts gathered at the WFITN meeting in Val d'Isère in 2007. Four paradigm unruptured aneurysms were used to poll opinions on risks of treatment or observation, as well as on their willingness to treat, observe or propose to the patient participation in a randomized trial, using six questions for each aneurysm. Opinions varied widely among lesions and among participants. Most participants (92.5%) were consistent, as they would offer treatment only if their estimate of the ten-year risk of spontaneous hemorrhage would exceed risks of treatment. Estimates of the natural history were consistently higher than that reported by ISUIA. Conversely, treatment risks were underestimated compared to those reported in ISUIA, but within the range reported in a recent French registry (ATENA). Participants were more confident in their evaluation of treatment risks and in their skills at treating aneurysms than in their estimates of risks of rupture entailed by the presence of the lesion, the latter being anchored at or close to 1%/year. The gulf between expert opinions, clinical practices and available data from registries persist. Expert opinions are compatible with the primary hypothesis of a recently initiated randomized trial on unruptured aneurysms (TEAM), which is a benefit of endovascular treatment of 4% compared to observation over ten years.Only data from a randomized trial could provide convincing objective evidence in favour or against preventive treatment of unruptured intracranial aneurysms.
Figures
Similar articles
-
Unruptured Intracranial Aneurysms. A Critical Review of the International Study of Unruptured Intracranial Aneurysms (ISUIA) and of Appropriate Methods to Address the Clinical Problem.Interv Neuroradiol. 2008 Mar 30;14(1):85-96. doi: 10.1177/159101990801400111. Epub 2008 May 12. Interv Neuroradiol. 2008. PMID: 20557790 Free PMC article.
-
Coil embolization for intracranial aneurysms: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(1):1-114. Epub 2006 Jan 1. Ont Health Technol Assess Ser. 2006. PMID: 23074479 Free PMC article.
-
Treatments for unruptured intracranial aneurysms.Cochrane Database Syst Rev. 2021 May 10;5(5):CD013312. doi: 10.1002/14651858.CD013312.pub2. Cochrane Database Syst Rev. 2021. PMID: 33971026 Free PMC article.
-
Age-related differences in unruptured intracranial aneurysms: 1-year outcomes.J Neurosurg. 2014 Nov;121(5):1024-38. doi: 10.3171/2014.6.JNS121179. Epub 2014 Aug 29. J Neurosurg. 2014. PMID: 25170670
-
Management of Unruptured Cerebral Aneurysms and Arteriovenous Malformations.Continuum (Minneap Minn). 2020 Apr;26(2):478-498. doi: 10.1212/CON.0000000000000835. Continuum (Minneap Minn). 2020. PMID: 32224762 Review.
Cited by
-
Growth and rupture of an intracranial aneurysm: the role of wall aneurysmal enhancement and CD68.Front Surg. 2023 Sep 6;10:1228955. doi: 10.3389/fsurg.2023.1228955. eCollection 2023. Front Surg. 2023. PMID: 37744724 Free PMC article.
-
Age- and gender-dependent variability in the geometry of middle cerebral artery bifurcations.J Anat. 2021 Mar;238(3):765-784. doi: 10.1111/joa.13338. Epub 2020 Oct 27. J Anat. 2021. PMID: 33107033 Free PMC article.
-
The TEAM trial: safety and efficacy of endovascular treatment of unruptured intracranial aneurysms in the prevention of aneurysmal hemorrhages: a randomized comparison with indefinite deferral of treatment in 2002 patients followed for 10 years.Trials. 2008 Jul 16;9:43. doi: 10.1186/1745-6215-9-43. Trials. 2008. PMID: 18631395 Free PMC article.
-
Endovascular treatment of unruptured intracranial aneurysms.Interv Neuroradiol. 2011 Dec;17(4):420-4. doi: 10.1177/159101991101700404. Epub 2011 Dec 16. Interv Neuroradiol. 2011. PMID: 22192544 Free PMC article.
-
"Sit back, observe, and wait." Or is there a pharmacologic preventive treatment for cerebral aneurysms?Neurosurg Rev. 2013 Jan;36(1):1-9; discussion 9-10. doi: 10.1007/s10143-012-0429-7. Epub 2012 Oct 16. Neurosurg Rev. 2013. PMID: 23070279 Review.
References
-
- Bacon F. First book: Of the proficience and advancement of learning, divine and human. Part V, section 8. 1605. 2004. Apr, The advancement of Learning. Available from the Gutenberg project: Release #5500. URL: http://www.gutenberg.org/wiki/Main_Page . Acessed June 29th, 2007.
-
- Wiebers DO, Whisnant JP, et al. Unruptured intracranial aneurysms: Natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003;362:103–110. - PubMed
-
- Tversky A, Kahneman D. Judgment under uncertainty: Heuristics and biaises. Science. 1974:1124–1131. - PubMed
-
- Rasmussen P, Mayberg M. Defining the natural history of unruptured aneurysms. Stroke. 2004;35:232–233. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
