

Procession to pediatric bacteremia and sepsis: covert operations and failures in diplomacy
- PMID: 20566606
- PMCID: PMC3142627
- DOI: 10.1542/peds.2009-3169
Procession to pediatric bacteremia and sepsis: covert operations and failures in diplomacy
Abstract
Despite advances in diagnosis and treatment, bacterial sepsis remains a major cause of pediatric morbidity and mortality, particularly among neonates, the critically ill, and the growing immunocompromised patient population. Sepsis is the end point of a complex and dynamic series of events in which both host and microbial factors drive high morbidity and potentially lethal physiologic alterations. In this article we provide a succinct overview of the events that lead to pediatric bloodstream infections (BSIs) and sepsis, with a focus on the molecular mechanisms used by bacteria to subvert host barriers and local immunity to gain access to and persist within the systemic circulation. In the events preceding and during BSI and sepsis, Gram-positive and Gram-negative pathogens use a battery of factors for translocation, inhibition of immunity, molecular mimicry, intracellular survival, and nutrient scavenging. Gaps in understanding the molecular pathogenesis of bacterial BSIs and sepsis are highlighted as opportunities to identify and develop new therapeutics.
Conflict of interest statement
Conflicts of Interest: None declared
Figures
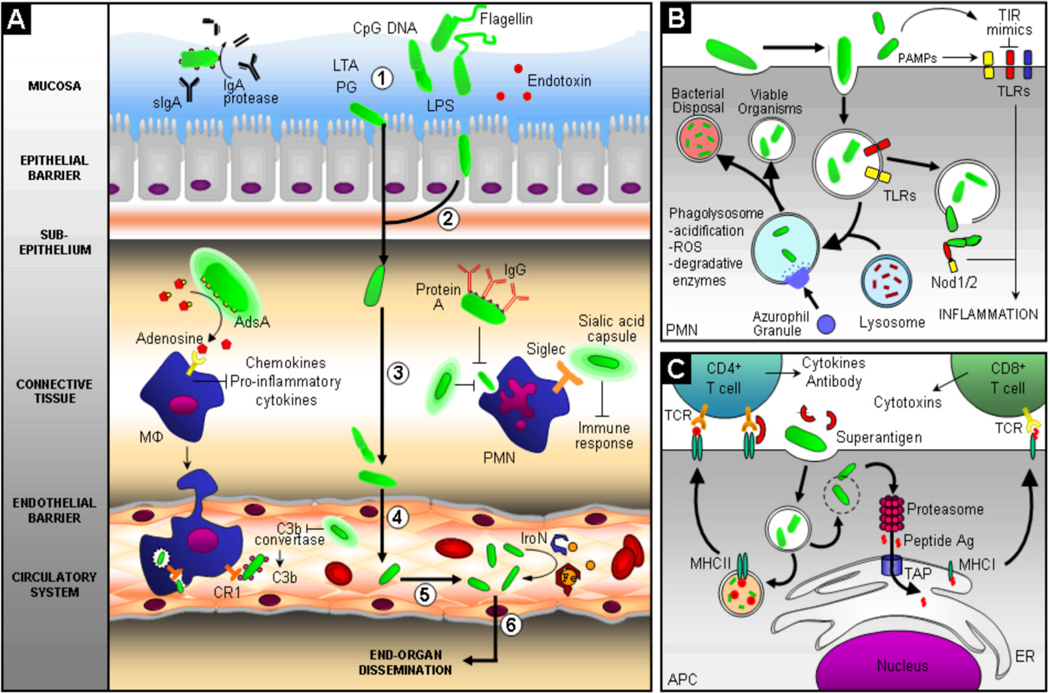
 ) indicates steps during the progression of BSI and sepsis; unbolded arrow (
) indicates steps during the progression of BSI and sepsis; unbolded arrow ( ) indicates activation of pathway; (
) indicates activation of pathway; ( ) indicates inhibition of pathway; curved unbolded arrow (
) indicates inhibition of pathway; curved unbolded arrow ( ) indicates production; MΦ, macrophage; PMN, polymorphonuclear neutrophil; LTA, lipotechoic acid; PG, petidoglycan; LPS, lipopolysaccharide; IgG, Immunoglobulin G; IgA, Immunoglobulin A; sIGA, secretory IgA; CR1, Complement Receptor 1; Fe, iron; IroN, siderophore; TIR, TLR/Interleukin-1 receptor; Nod1/2, cytoplasmic PAMP receptors; ROS, reactive oxygen species; TCR, T cell receptor; TAP, transporter associated with antigen processing; ER, endoplasmic reticulum; APC, antigen presenting cell; MHCI/II, major histocompatability complex I/II; Ag, antigen; CD4+, T cell co-receptor distinguishing T helper cells; CD8+ T cell co-receptor distinguishing cytotoxic T cells.
) indicates production; MΦ, macrophage; PMN, polymorphonuclear neutrophil; LTA, lipotechoic acid; PG, petidoglycan; LPS, lipopolysaccharide; IgG, Immunoglobulin G; IgA, Immunoglobulin A; sIGA, secretory IgA; CR1, Complement Receptor 1; Fe, iron; IroN, siderophore; TIR, TLR/Interleukin-1 receptor; Nod1/2, cytoplasmic PAMP receptors; ROS, reactive oxygen species; TCR, T cell receptor; TAP, transporter associated with antigen processing; ER, endoplasmic reticulum; APC, antigen presenting cell; MHCI/II, major histocompatability complex I/II; Ag, antigen; CD4+, T cell co-receptor distinguishing T helper cells; CD8+ T cell co-receptor distinguishing cytotoxic T cells.References
-
- Jean-Baptiste E. Cellular mechanisms in sepsis. J Intensive Care Med. 2007;22(2):63–72. - PubMed
-
- Watson RS, Carcillo JA, Linde-Zwirble WT, Clermont G, Lidicker J, Angus DC. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med. 2003;167(5):695–701. - PubMed
-
- Wisplinghoff H, Seifert H, Tallent SM, Bischoff T, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in pediatric patients in United States hospitals: epidemiology, clinical features and susceptibilities. Pediatr Infect Dis J. 2003;22(8):686–691. - PubMed
-
- Bizzarro MJ, Raskind C, Baltimore RS, Gallagher PG. Seventy-five years of neonatal sepsis at Yale: 1928–2003. Pediatrics. 2005;116(3):595–602. - PubMed
-
- Lee CY, Chen PY, Huang FL, Lin CF. Microbiologic spectrum and susceptibility pattern of clinical isolates from the pediatric intensive care unit in a single medical center - 6 years' experience. J Microbiol Immunol Infect. 2009;42(2):160–165. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
