

Micronutrient fortification to improve growth and health of maternally HIV-unexposed and exposed Zambian infants: a randomised controlled trial
- PMID: 20567511
- PMCID: PMC2887362
- DOI: 10.1371/journal.pone.0011165
Micronutrient fortification to improve growth and health of maternally HIV-unexposed and exposed Zambian infants: a randomised controlled trial
Abstract
Background: The period of complementary feeding, starting around 6 months of age, is a time of high risk for growth faltering and morbidity. Low micronutrient density of locally available foods is a common problem in low income countries. Children of HIV-infected women are especially vulnerable. Although antiretroviral prophylaxis can reduce breast milk HIV transmission in early infancy, there are no clear feeding guidelines for after 6 months. There is a need for acceptable, feasible, affordable, sustainable and safe (AFASS by WHO terminology) foods for both HIV-exposed and unexposed children after 6 months of age.
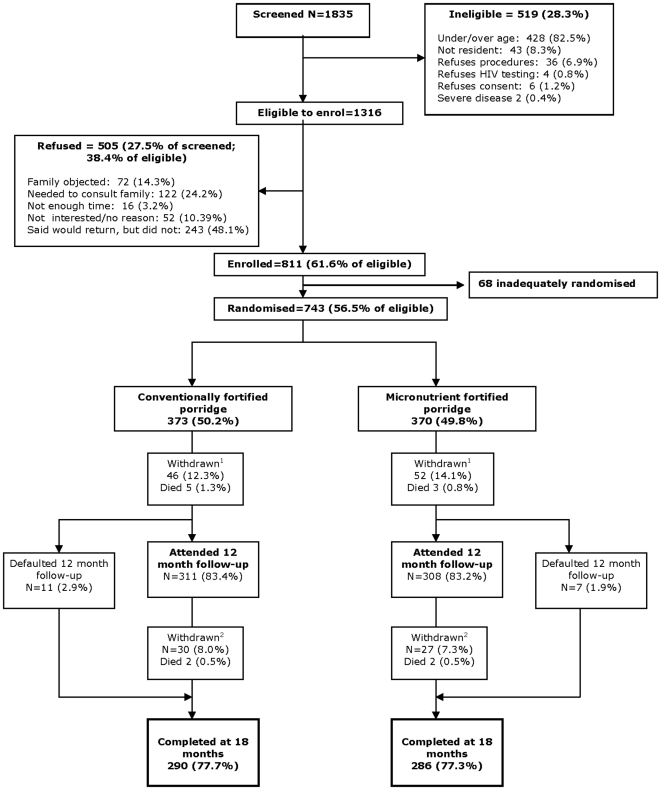
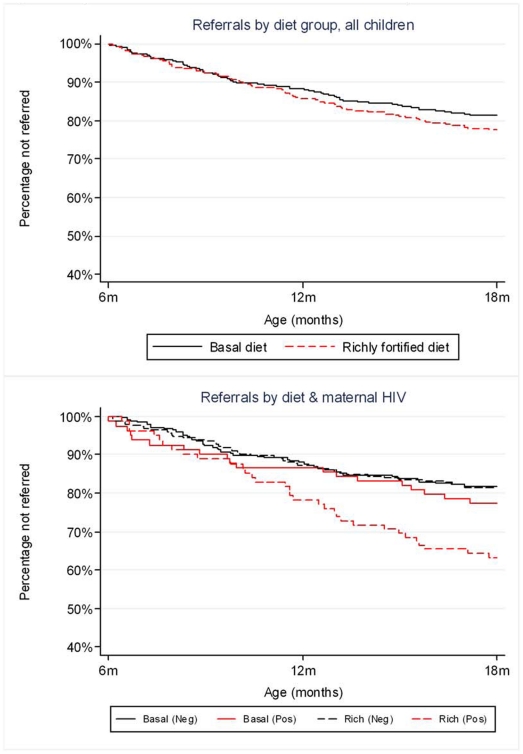
Methods and findings: We conducted in Lusaka, Zambia, a randomised double-blind trial of two locally made infant foods: porridges made of flour composed of maize, beans, bambaranuts and groundnuts. One flour contained a basal and the other a rich level of micronutrient fortification. Infants (n = 743) aged 6 months were randomised to receive either regime for 12 months. The primary outcome was stunting (length-for-age Z<-2) at age 18 months. No significant differences were seen between trial arms overall in proportion stunted at 18 months (adjusted odds ratio 0.87; 95% CI 0.50, 1.53; P = 0.63), mean length-for-age Z score, or rate of hospital referral or death. Among children of HIV-infected mothers who breastfed <6 months (53% of HIV-infected mothers), the richly-fortified porridge increased length-for-age and reduced stunting (adjusted odds ratio 0.17; 95% CI 0.04, 0.84; P = 0.03). Rich fortification improved iron status at 18 months as measured by hemoglobin, ferritin and serum transferrin receptors.
Conclusions: In the whole study population, the rich micronutrient fortification did not reduce stunting or hospital referral but did improve iron status and reduce anemia. Importantly, in the infants of HIV-infected mothers who stopped breastfeeding before 6 months, the rich fortification improved linear growth. Provision of such fortified foods may benefit health of these high risk infants.
Trial registration: Controlled-Trials.com ISRCTN37460449.
Conflict of interest statement
Figures
References
-
- Shrimpton R, Victora C, de Onis M, Lima R, Blössner M, et al. Worldwide timing of growth faltering: implications for nutritional interventions. Pediatrics. 2001;107:e75. - PubMed
-
- World Health Organization. 2001. The optimal duration of exclusive breastfeeding.
-
- World Health Organization. 2002. Complementary feeding: Summary of guiding principles for complementary feeding of the breastfed child.
-
- Filteau S. The HIV-exposed, uninfected African child. Trop Med Int Health. 2009;14:276–287. - PubMed
-
- World Health Organization. 2007. HIV and infant feeding: update.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
