

Lip reconstruction
- PMID: 20567703
- PMCID: PMC2884873
- DOI: 10.1055/s-0028-1095886
Lip reconstruction
Abstract
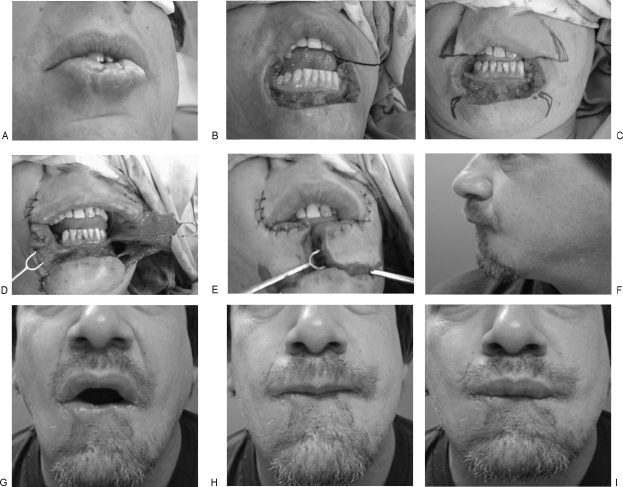
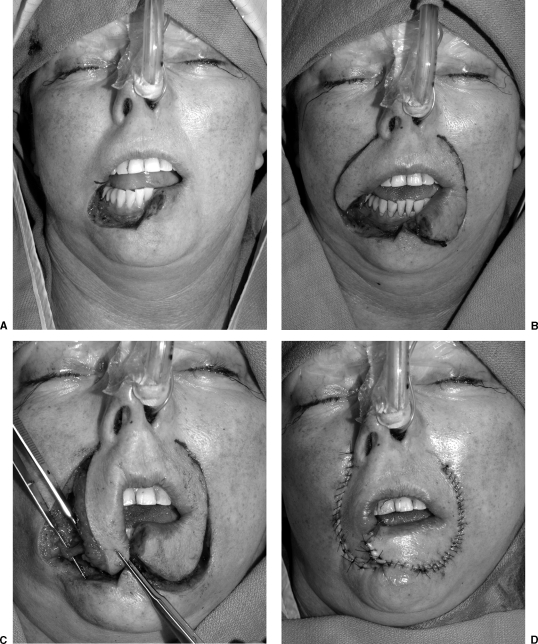
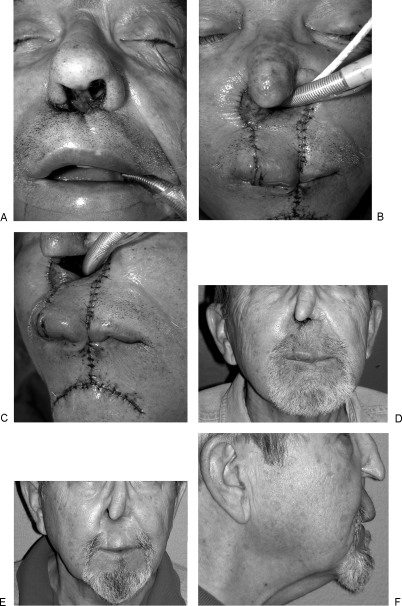
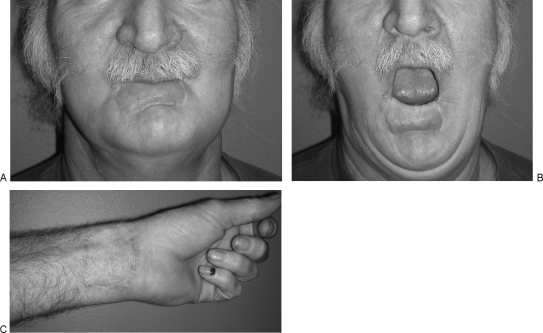
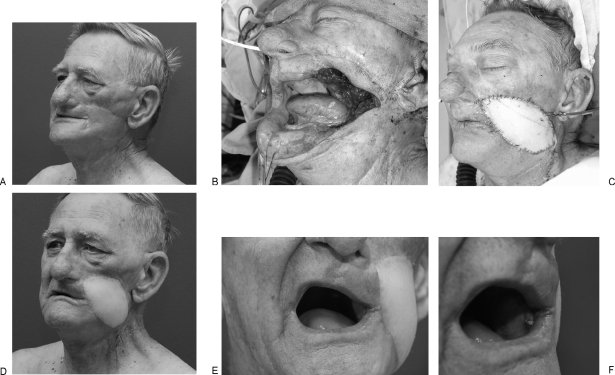
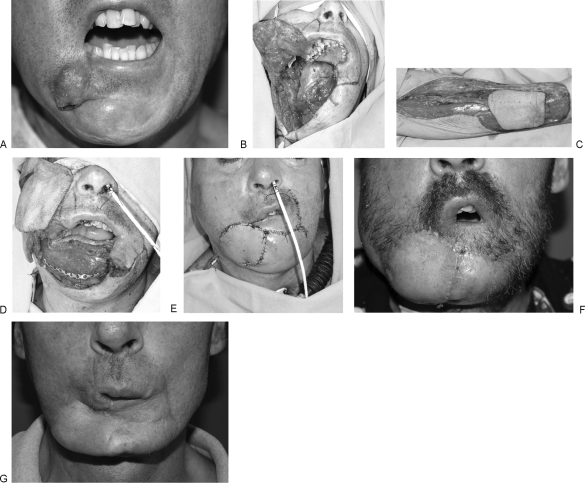
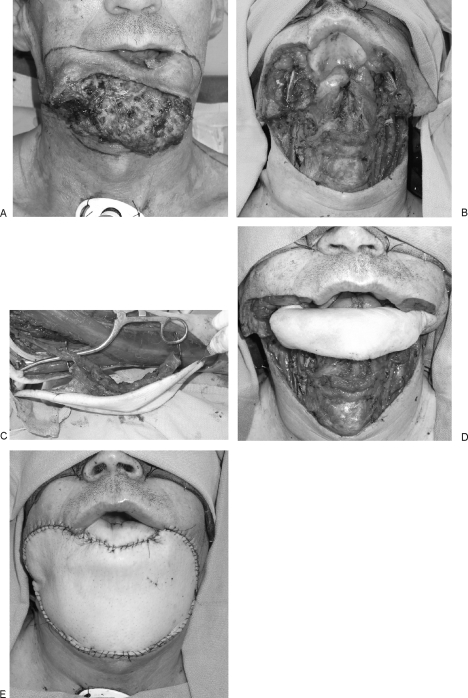
Lip reconstruction poses a particular challenge to the plastic surgeon in that the lips are the dynamic center of the lower third of the face. Their role in aesthetic balance, facial expression, speech, and deglutination is not replicated by any other tissue substitute. The goals of lip reconstruction are both functional and aesthetic, and the surgical techniques employed are often overlapping. This discussion will focus on lip defects with significant tissue loss that require flap reconstruction. Flaps described include Webster-Bernard cheek advancement flaps, Abbe cross-lip flaps, Karapandzic rotation advancement flaps, and single and dual free-flap lip reconstructions. The principles and techniques described are broadly applicable to other flap designs that are required to meet both the aesthetic and functional goals of lip reconstruction.
Keywords: Abbe flap; Karapandzic flap; Lip reconstruction; Webster-Bernard flap; free flap.
Figures



References
-
- Adams W, Beran S. Lip, cheek, and scalp reconstruction; hair replacement. Selected Readings in Plastic Surgery. 2001;15:2–16.
-
- Kroll S. In: Kroll S, editor. Reconstructive Plastic Surgery for Cancer. St. Louis, MO: Mosby Year Book; 1996. Lip reconstruction. pp. 201–209.
-
- Webster R C, Coffey R J, Kelleher R E. Total and partial reconstruction of the lower lip with innervated muscle-bearing flaps. Plast Reconstr Surg Transplant Bull. 1960;25:360–371. - PubMed
-
- Closmann J J, Pogrel M A, Schmidt B L. Reconstruction of perioral defects following resection for oral squamous cell carcinoma. J Oral Maxillofac Surg. 2006;64:367–374. - PubMed
-
- Langstein H N, Robb G L. Lip and perioral reconstruction. Clin Plast Surg. 2005;32:431–445. - PubMed
