

doi: 10.1055/s-2008-1081398.
Reconstruction of head and neck defects: a systematic approach to treatment
Affiliations
- PMID: 20567709
- PMCID: PMC2884883
- DOI: 10.1055/s-2008-1081398
Item in Clipboard
Reconstruction of head and neck defects: a systematic approach to treatment
Semin Plast Surg.
2008 Aug.
Abstract
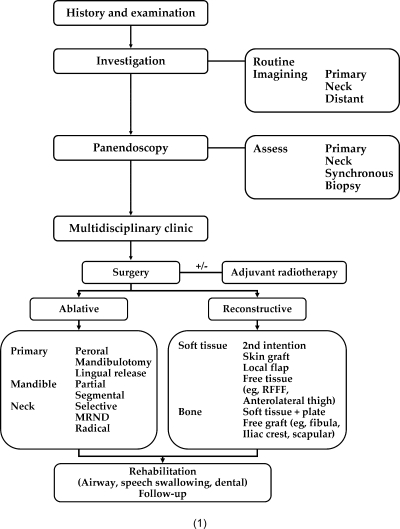
Reconstruction of composite maxillofacial defects after tumor excision or trauma is difficult. The role of the reconstructive surgeon is to have a diverse armamentarium of reconstructive options to enable an aesthetic and functional reconstruction while minimizing the morbidity to the patient. This article will present a systematic review of composite maxillofacial reconstruction with free tissue transfer.
Keywords: Reconstruction; mandible; maxilla; osteocutaneous free flaps.
Figures
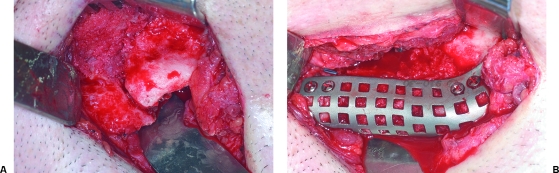
(A) Left mandible pathologic fracture secondary to elective third molar removal. Multiple transoral attempts at bone grafting failed due to intraoral dehiscence. (B) Definitive reconstruction was performed with nonvascularized iliac crest bone graft with titanium mesh tray.
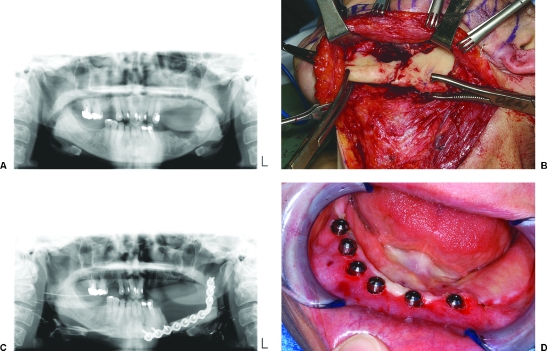
(A) Osteoradionecrosis of left mandible with pathologic fracture. (B) It is treated with resection and immediate free fibula osteocutaneous flap reconstruction. (C) Postoperative panoramic radiograph after free fibula flap reconstruction. (D) Secondary placement of osseointegrated dental implants into native mandible after indentialation of remaining teeth. Note the excellent contour of the skin paddle used for intraoral lining.

(A) Patient sustained a ballistic injury to the face with a comminuted right body and symphysis mandibular fracture treated elsewhere with multiple failed attempts at nonvascularized iliac crest bone grafting. (B) Patient developed an orocutaneous fistula to the mandibular hardware. Patient treated with a single-stage resection and immediate reconstruction with osteocutaneous fibula free flap with extraoral skin paddle for resurfacing the neck.
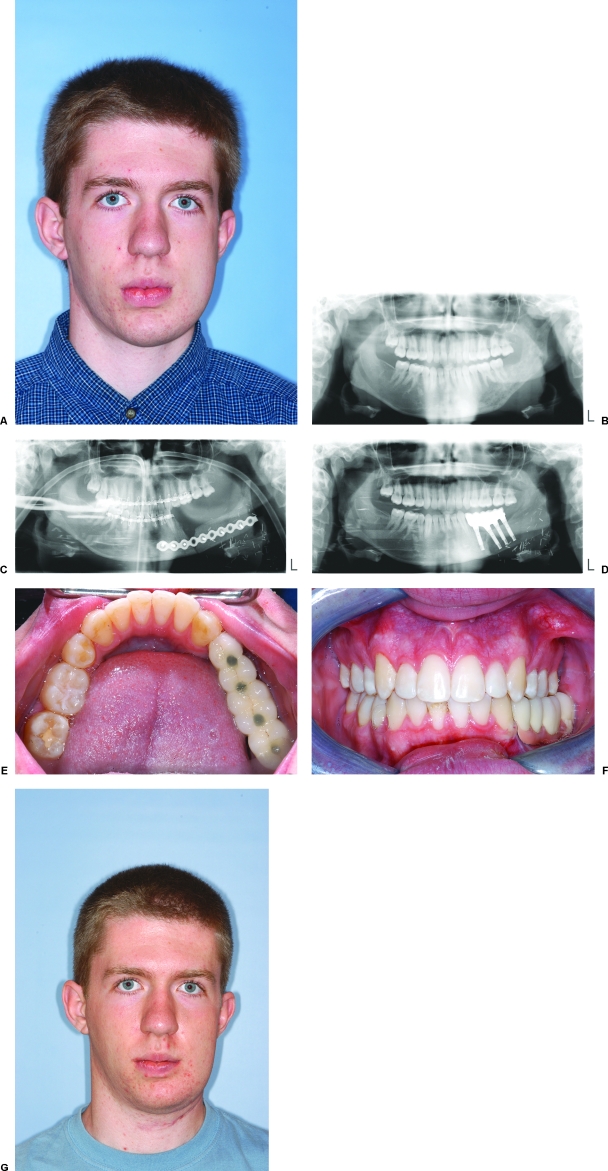
(A) Patient with refractory acute/chronic osteomyelitis resistant to medical therapy. (B) Preoperative panoramic radiograph. (C) Patient was treated with a single-stage hemimandibular resection and immediate reconstruction with vascularized iliac crest free flap. (D) Secondary-stage procedure was performed for placement of osseointegrated dental implants. (E) Postoperative occlusal view of mandible. Note the bone volume is close to the native mandible. (F) Completed final occlusion. Note the excellent facial symmetry (A) before and (G) after surgery and occlusion achieved with prosthetic reconstruction.
(A) Patient with advanced-stage T4 tumor of the retromolar trigone with involvement of the adjacent tongue and floor of the mouth. In oncologic tongue defects greater than one-half the lateral border of the tongue, for optimal tongue motion, a dual free flap approach can be considered. (B) Preoperative panoramic radiograph. (C) This case was reconstructed with a free fibula osseous free flap for mandible reconstruction with a radial forearm free flap for tongue and floor of mouth reconstruction. Patient has excellent speech and was able to take oral alimentation in the immediate postoperative period.
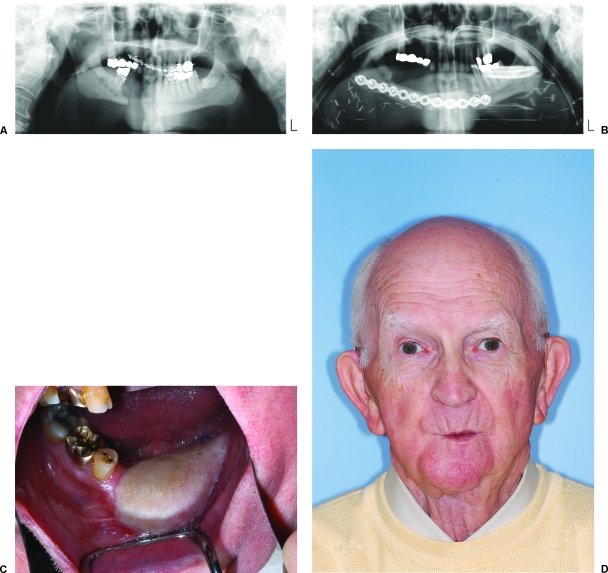
(A) Elderly patient who presented with a mandibular defect after undergoing several attempts at nonvascularized bone grafting elsewhere. Both anterior and posterior iliac crest sites previously used. (B) Postoperative panoramic radiograph. (C) Patient treated with osteocutaneous free fibula with skin paddle for intraoral resurfacing. (D) Postoperative facial appearance. He did not want to pursue prosthetic reconstruction therefore did not undergo osseointegrated dental implant placement.
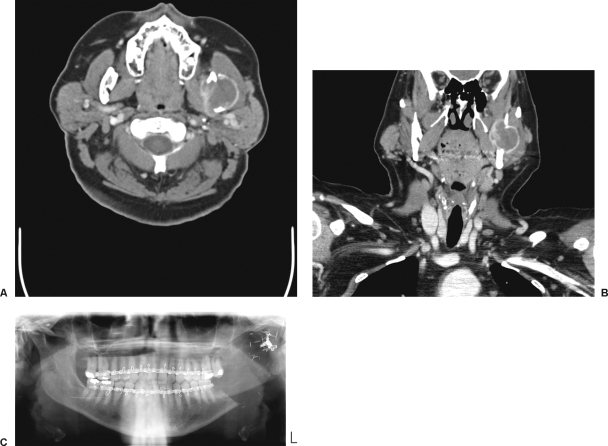
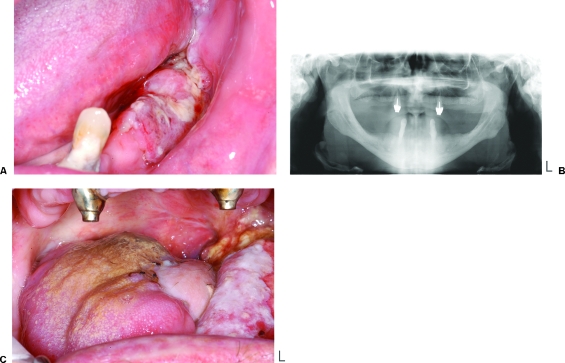
(A–C) Patient with a high-grade angiosarcoma of the mandible. Patient underwent resection via a transfacial, transparotid approach. No immediate reconstruction was performed due to patient's refusal of blood product transfusion. Left mandible disarticulated. Patient functioned without formal reconstruction and does not desire definitive reconstruction. (A) Axial CT. (B) Coronal CT. (C) Postoperative panoramic radiograph of mandible.
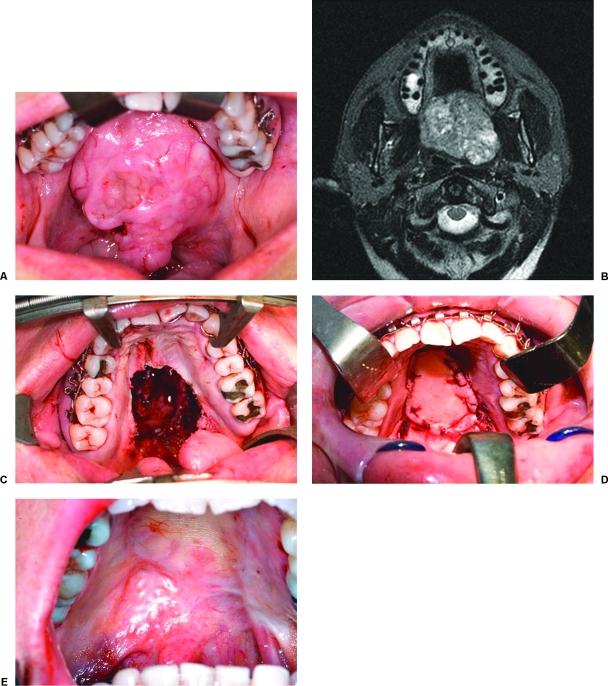
(A) Patient with a large pleomorphic adenoma of the palate left untreated for several years. Patient was unwilling to wear a prosthetic obturator and therefore underwent resection with immediate reconstruction with radial forearm fasciocutaneous free flap. This provided restoration of anatomic form with excellent functional results. (B) Axial CT showing large mass in the palatal and lateral pharyngeal space. (C) Transoral maxillectomy allowing unblocked tumor removal with postoperative defect. (D) Radial forearm free flap inset for defect reconstruction. (E) Six month postoperative appearance of the palate.
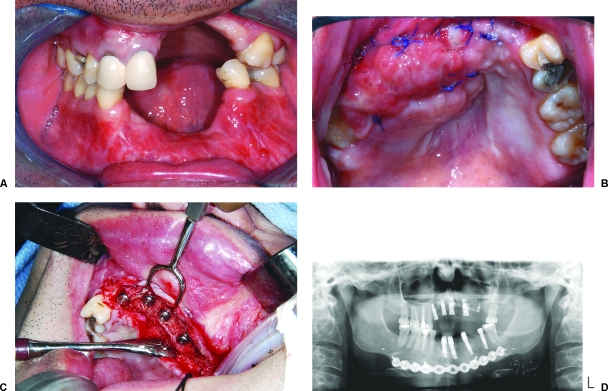
(A) Limited alveolar defect secondary to ballistic injury with insufficient soft tissue envelope to allow nonvascularized bone grafting. (B) Reconstructed with medial femoral periosteal free flap. (C) Delayed placement of osseointegrated dental implants into flap. Note the periosteal payer was inset to the oral mucosa and allowed to mucosalize over a period of 6 weeks. (D) Postoperative panorex showing incorporation of bone.
References
-
- Gilbert A. Vascularized transfer of the fibula shaft. Int J Microsurg. 1979;1:100.
-
- Gilbert A, Teot L. The free scapular flap. Plast Reconstr Surg. 1982;69:601–604. - PubMed
-
- Hidalgo D. Fibula free flap; a new method of mandible reconstruction. Plast Reconstr Surg. 1989;84:71–79. - PubMed
-
- Manchester W. Immediate reconstruction of the mandible and the TMJ. Br J Plast Surg. 1965;18:291–303. - PubMed
-
- Taylor G, Miller D FJH. The free vascularized bone graft: a clinical extension of microvascular techniques. Plast Reconstr Surg. 1975;55:533–544. - PubMed
