

doi: 10.1055/s-0029-1214159.
Osteomyelitis of the craniofacial skeleton
Affiliations
- PMID: 20567729
- PMCID: PMC2884909
- DOI: 10.1055/s-0029-1214159
Item in Clipboard
Osteomyelitis of the craniofacial skeleton
Semin Plast Surg.
2009 May.
Abstract
Skull-based osteomyelitis, which is a true bony infection, originates from a chronic, inadequately treated infection. Because of the complex craniofacial skeletal anatomy and associated aesthetic concerns, osteomyelitis of the craniofacial skeleton must be uniquely managed and is more difficult to treat than osteomyelitis of other bones of the body. It is thought that osteomyelitis is decreasing in prevalence due to broad-spectrum antibiotic treatment; however, it still remains a challenging clinical entity in developing countries and lower socioeconomic areas.
Keywords: Osteomyelitis; craniofacial infection; head and neck; osteomyelitis of the mandible; skull base.
Figures
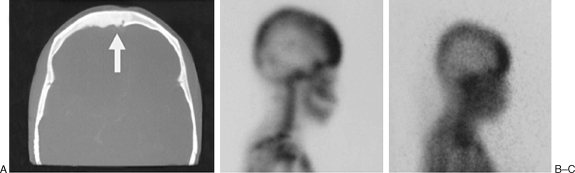
(A) A CT scan with frontal sinus inflammation. (B) Scintigraphy with inflammatory activity and osteomyelitis (99mTc). (C) Scintigraphy with inflammatory activity and osteomyelitis (67Ga).

(A) Sagittal T1-weighted image demonstrates abnormally low signal intensity in the inferior clivus. (B) Axial T1-weighted image demonstrates abnormal soft tissue isointense to muscle infiltrating submucosally within the nasopharyngeal soft tissues, extending posteriorly to abut the carotid arteries (arrowheads), and replacing the normal hyperintense fatty marrow within the lower clivus. (C) Axial T2-weighted fast spin-echo image with fat saturation demonstrates mildly increased signal intensity within the infiltrated soft tissue compared with that of normal muscle. In addition, there is fluid in the mastoid air cells and middle ear cavities bilaterally, presumably related to Eustachian tube dysfunction or obstruction or both. (D) Contrast-enhanced axial T1-weighted spin-echo image with fat saturation demonstrates moderately intense enhancement of the infiltrative soft tissue. Some areas of nonenhancement may represent areas of infarcted or necrotic muscle. (E) Axial T1-weighted spin-echo image from a follow-up MR examination 16 months after the initial study demonstrates normalization of clival signal intensity (white arrows), as well as considerable reduction in bulk of the previously noted abnormal pre- and paraclival soft tissue. (F) Contrast-enhanced axial T1-weighted spin-echo image with fat saturation from the same follow-up examination demonstrates marked reduction of enhancement, with a normal appearance to the nasopharynx and prevertebral muscles. An ill-defined area of linear enhancement just at and anterior to the hypoglossal canal on the right (arrow) is likely extending along the course of the hypoglossal nerve. Of note, this patient's hypoglossal palsy has persisted despite resolution of all other symptoms. (Figure and description from Chang PC, Fischbein NJ, Holliday RA. Central skull base osteomyelitis in patients without otitis externa: imaging findings. AJNR Am J Neuroradiol 2003;24:1310–1316. Copyright © by American Society of Neuroradiology. Reprinted with permission.)
References
-
- Prasad K C, Prasad S C, Mouli N, Agarwal S. Osteomyelitis in the head and neck. Acta Otolaryngol. 2007;127:194–205. - PubMed
-
- In: Peterson L, editor. Contemporary Oral Maxillofacial Surgery. 4th ed. Philadelphia,PA: Mosby Publishers; 2003. Osteomyelitis. pp. 375–377.
-
- Strumas N, Antonyshyn O, Caldwell C B, Mainprize J. Multimodality imaging for precise localization of craniofacial osteomyelitis. J Craniofac Surg. 2003;14:215–219. - PubMed
-
- Wallace-Hudson J. In: Fonseca RJ, editor. Oral and Maxillofacial Surgery: Surgical Pathology. Philadelphia, PA: WB Saunders; 2000. Osteomyelitis and osteoradionecrosis. pp. 484–490.
