

Reconstruction of osteomyelitis defects of the craniofacial skeleton
- PMID: 20567734
- PMCID: PMC2884900
- DOI: 10.1055/s-0029-1214164
Reconstruction of osteomyelitis defects of the craniofacial skeleton
Abstract
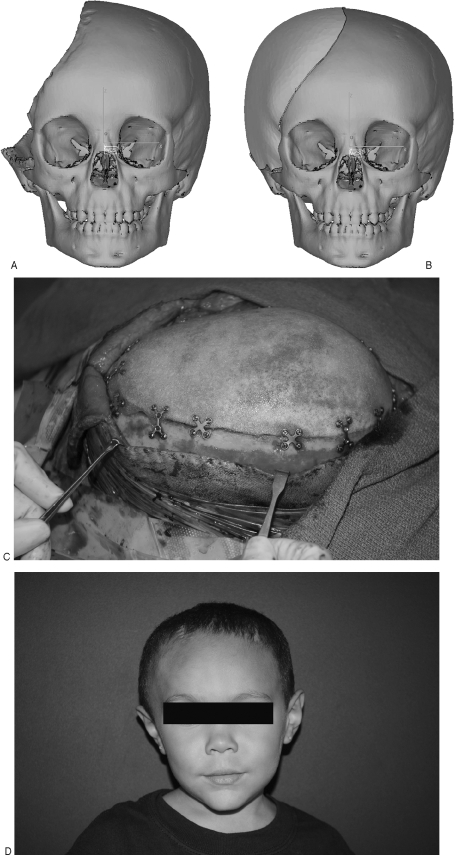
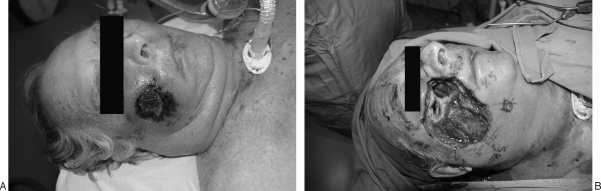
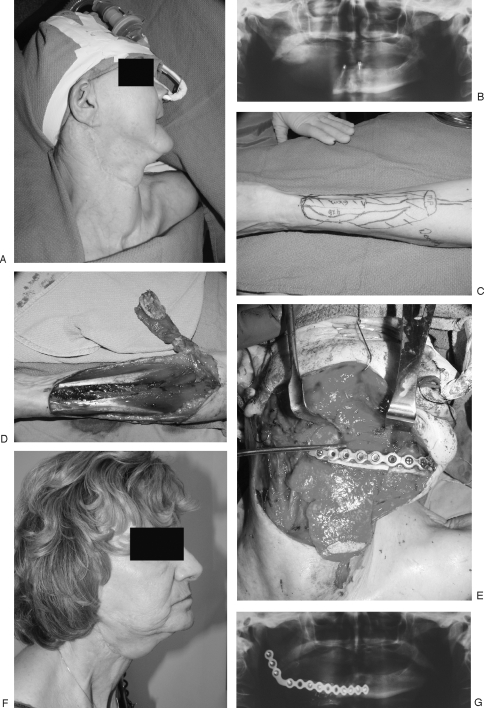
Osteomyelitis of the craniofacial skeleton closely resembles osteomyelitis elsewhere in the body in its pathophysiology and medical management; subsequent reconstruction after debridement remains distinctly challenging. The goals of reconstruction must include the restoration of the complex and readily visible morphology of the cranium and face, as well as the adequate return of vital sensory, expressive, and digestive functions. In this article, the various reconstructive modalities will be discussed including pedicled and nonpedicled flaps with or without an osseous component, nonvascularized bone grafts, alloplastic implants, and bone regeneration using protein therapy. Although reconstruction of craniofacial defects after osteomyelitis commonly proves formidable, the satisfactory return of form and function remains a plausible reconstructive goal.
Keywords: Osteomyelitis; craniofacial; head and neck; mandible; midface; reconstruction; skull.
Figures




References
-
- Nelaton A. Elements De Pathologie Chirurgicale. Paris, France: Germer-Bailliere; pp. 1844–1859.
-
- David D J, Cooter R D. Craniofacial infection in 10 years of transcranial surgery. Plast Reconstr Surg. 1987;80:213–225. - PubMed
-
- Fearon J A, Yu J, Bartlett S P, Munro I R, Chir B, Whitaker L. Infections in craniofacial surgery: a combined report of 567 procedures from two centers. Plast Reconstr Surg. 1997;100:862–868. - PubMed
-
- Barker F G., II Efficacy of prophylactic antibiotics for craniotomy: a meta-analysis. Neurosurgery. 1994;35:484–490. discussion 491–482. - PubMed
-
- Verbon A, Husni R N, Gordon S M, Lavertu P, Keys T F. Pott's puffy tumor due to Haemophilus influenzae: case report and review. Clin Infect Dis. 1996;23:1305–1307. - PubMed
