

Sagittal plane deformity: an overview of interpretation and management
- PMID: 20567858
- PMCID: PMC2989270
- DOI: 10.1007/s00586-010-1476-9
Sagittal plane deformity: an overview of interpretation and management
Abstract
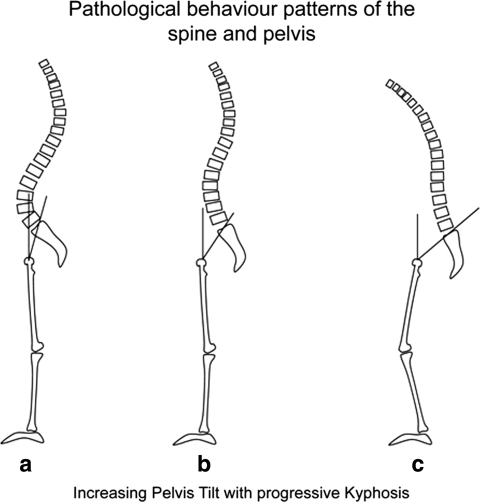
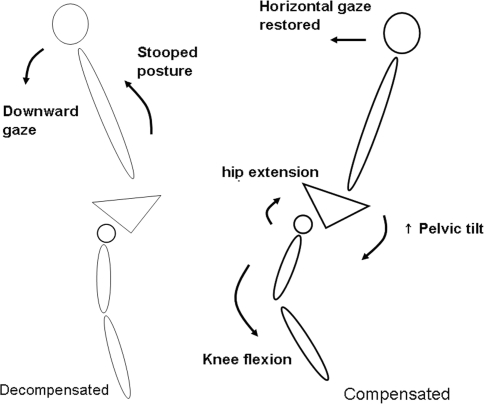
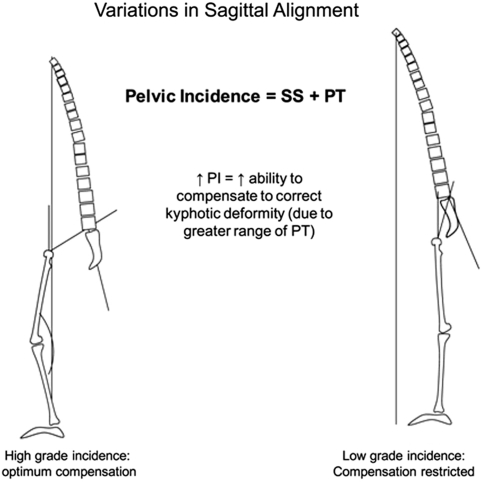
The impact of sagittal plane alignment on the treatment of spinal disorders is of critical importance. A failure to recognise malalignment in this plane can have significant consequences for the patient not only in terms of pain and deformity, but also social interaction due to deficient forward gaze. A good understanding of the principles of sagittal balance is vital to achieve optimum outcomes when treating spinal disorders. Even when addressing problems in the coronal plane, an awareness of sagittal balance is necessary to avoid future complications. The normal spine has lordotic curves in the cephalad and caudal regions with a kyphotic curve in between. Overall, there is a positive correlation between thoracic kyphosis and lumbar lordosis. There are variations on the degree of normal curvature but nevertheless this shape allows equal distribution of forces across the spinal column. It is the disruption of this equilibrium by pathological processes or, as in most cases, ageing that results in deformity. This leads to adaptive changes in the pelvis and lower limbs. The effects of limb alignment on spinal posture are well documented. We now also know that changes in pelvic posture also affect spinal alignment. Sagittal malalignment presents as an exaggeration or deficiency of normal lordosis or kyphosis. Most cases seen in clinical practise are due to kyphotic deformity secondary to inflammatory, degenerative or post-traumatic disorders. They may also be secondary to infection or tumours. There is usually pain and functional disability along with concerns about self-image and social interaction due to inability to maintain a horizontal gaze. The resultant pelvic and lower limb posture is an attempt to restore normal alignment. Addressing this complex problem requires detailed expertise and awareness of the potential pitfalls surrounding its treatment.
Figures

References
-
- Boesker EH, Moe JH, Winter RB, Koop SE. A determination of the normal thoracic kyphosis: a roentgenographic study of 121 normal children. J Pediatr Orthop. 2000;20:796–798. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
