

Carotid-cavernous fistula in ehlers-danlos syndrome by pure transvenous approach
- PMID: 20569551
- PMCID: PMC3355357
- DOI: 10.1177/159101990601200109
Carotid-cavernous fistula in ehlers-danlos syndrome by pure transvenous approach
Abstract
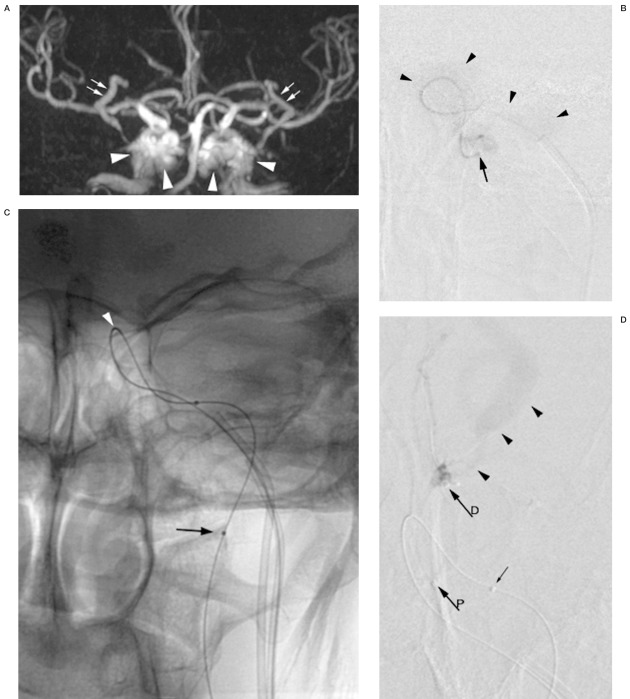
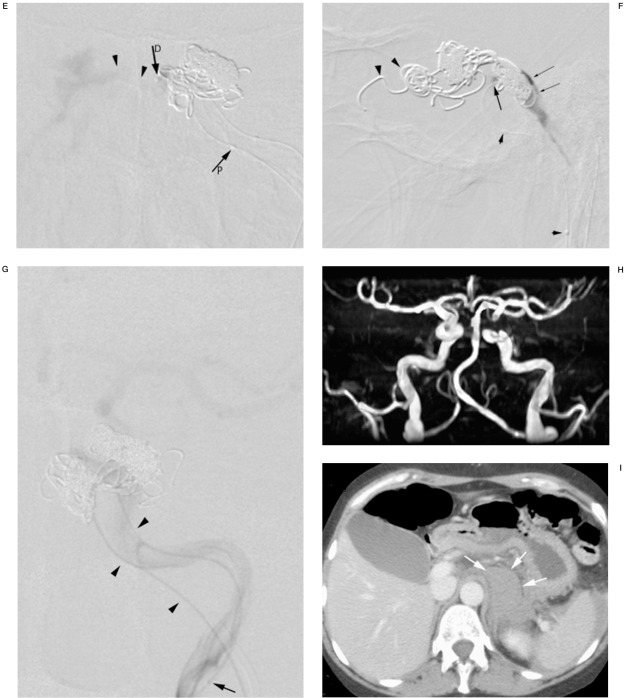
We describe a carotid-cavernous fistula (CCF) in a middle aged woman with Ehlers-Danlos syndrome (EDS) type IV, which manifested with a left-sided ophthalmoplegia. The CCF was diagnosed on magnetic resonance imaging. To prevent potential lethal arterial wall injury, the CCF was treated endovascularly under local anesthesia and exclusively by a transvenous approach. The fistula was successfully closed with Guglielmi Detachable Coils. Notwithstanding these precautionary measures, the patient suffered an intraperitoneal and a small retroperitoneal bleed during the procedure and died suddenly ten days after intervention in hemorrhagic shock. A review of recent literature focussing on the technique of transvenous approach and the catheterization risks of CCF in Ehlers-Danlos syndrome is presented.
Figures
References
-
- Beighton P, De Paepe A, et al. Ehlers-Danlos syndromes: revised nosology, Villefranche, 1997. Ehlers-Danlos National Foundation (USA) and Ehlers-Danlos Support Group (UK) Am J Med Genet. 1998;77:31–37. - PubMed
-
- De Paepe A, Malfait F. Bleeding and bruising in patients with Ehlers-Danlos syndrome and other collagen vascular disorders. Br J Haematol. 2004;127:491–500. - PubMed
-
- Citron SJ, Wallace RC, et al. Quality improvement guidelines for adult diagnostic neuroangiography: cooperative study between ASITN, ASNR, and SIR. J Vasc Interv Radiol. 2003;14:S257–262. - PubMed
-
- Schievink WI, Piepgras DG, et al. Spontaneous carotid-cavernous fistulae in Ehlers-Danlos syndrome Type IV. Case report. J Neurosurg. 1991;74:991–998. - PubMed
-
- Lach B, Nair SG, et al. Spontaneous carotid-cavernous fistula and multiple arterial dissections in type IV Ehlers-Danlos syndrome. Case report. J Neurosurg. 1987;66:462–467. - PubMed
LinkOut - more resources
Full Text Sources
