

Neurovascular radiosurgery
- PMID: 20569572
- PMCID: PMC3354536
- DOI: 10.1177/159101990601200301
Neurovascular radiosurgery
Abstract
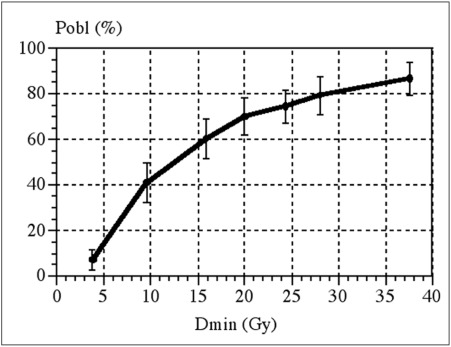
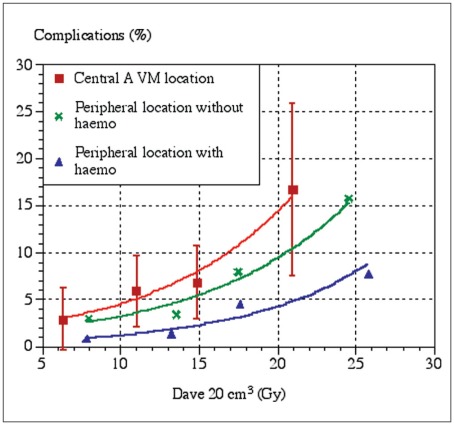
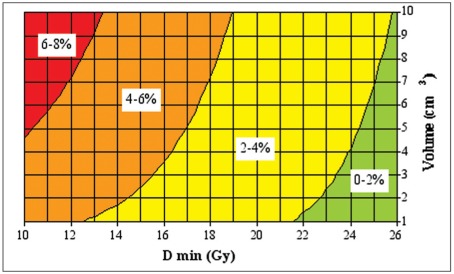
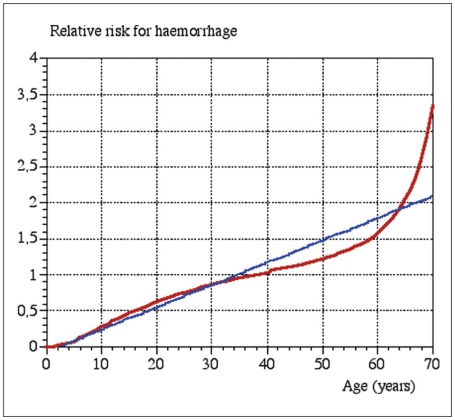
This article focuses on the treatment of neurovascular diseases, in particular brain arteriovenous malformations (BAVMs), with radiosurgery. The target group for this review is physicians who manage patients with neurovascular diseases, but are not actively engaged in radiosurgery. Radiosurgery for BAVMs is an established treatment with clearly defined risks and benefits. The efficacy of radiosurgery for dural arteriovenous shunts (DAVSs) is probably similar but the treatment has not yet gained the same acceptance. Radiosurgical treatment of cavernomas (cavernous hemangiomas) remains controversial. Well founded predictive models for BAVM radiosurgery show: * The probability of obliteration depends on the dose of radiation given to the periphery of the BAVM. * The risk of adverse radiation effects depends on the total dose of radiation, i.e. the amount of energy imparted into the tissue. The risk is greater in centrally located lesions. The risk of damage to brainstem nucleii and cranial nerves must be added to the risk predicted from current outcome models. * The risk of hemorrhage during the time span before obliteration depends on the BAVM volume, the dose of radiation to the periphery of the lesion and the age of the patient. Central location is a probably also a risk factor.
Figures
References
-
- Hillman J. Population-based analysis of arteriovenous malformation treatment. J Neurosurg. 2001;95(4):633–637. - PubMed
-
- Jellinger K. Vascular malformations of the central nervous system: a morphological overview. Neurosurg Rev. 1986;9(3):177–216. - PubMed
-
- Karhunen PJ, Penttila A, Erkinjuntti T. Arteriovenous malformation of the brain: imaging by postmortem angiography. Forensic Sci Int. 1990;48(1):9–19. - PubMed
-
- Wikholm G, Lundqvist C, Svendsen P. Embolization of cerebral arteriovenous malformations: Part I-Technique, morphology, and complications. Neurosurgery. 1996;39(3):448–457. discussion 457-459. - PubMed
-
- Ondra SL, Troupp H, et al. The natural history of symptomatic arteriovenous malformations of the brain: a 24-year follow up assessment. Journal of Neurosurgery. 1990;73:387–391. - PubMed
LinkOut - more resources
Full Text Sources
