

Review
doi: 10.1016/j.clp.2010.02.002.
Group B streptococcal disease in infants: progress in prevention and continued challenges
Affiliations
- PMID: 20569813
- PMCID: PMC11848810
- DOI: 10.1016/j.clp.2010.02.002
Item in Clipboard
Review
Group B streptococcal disease in infants: progress in prevention and continued challenges
Clin Perinatol.
2010 Jun.
Abstract
The burden of early-onset disease caused by group B Streptococcus (GBS) has decreased dramatically in the United States over the past 20 years. Universal culture-based screening at 35 to 37 weeks gestational age and use of intrapartum antibiotic prophylaxis are the cornerstones of prevention measures that have led to this decline. GBS, however, remains the leading cause of early-onset neonatal sepsis in the United States. Revised guidelines for prevention of perinatal GBS are planned for issuance in 2010. This article discusses implementation challenges for clinicians caring for pregnant women and newborns and presents an updated algorithm for neonatal management.
Figures
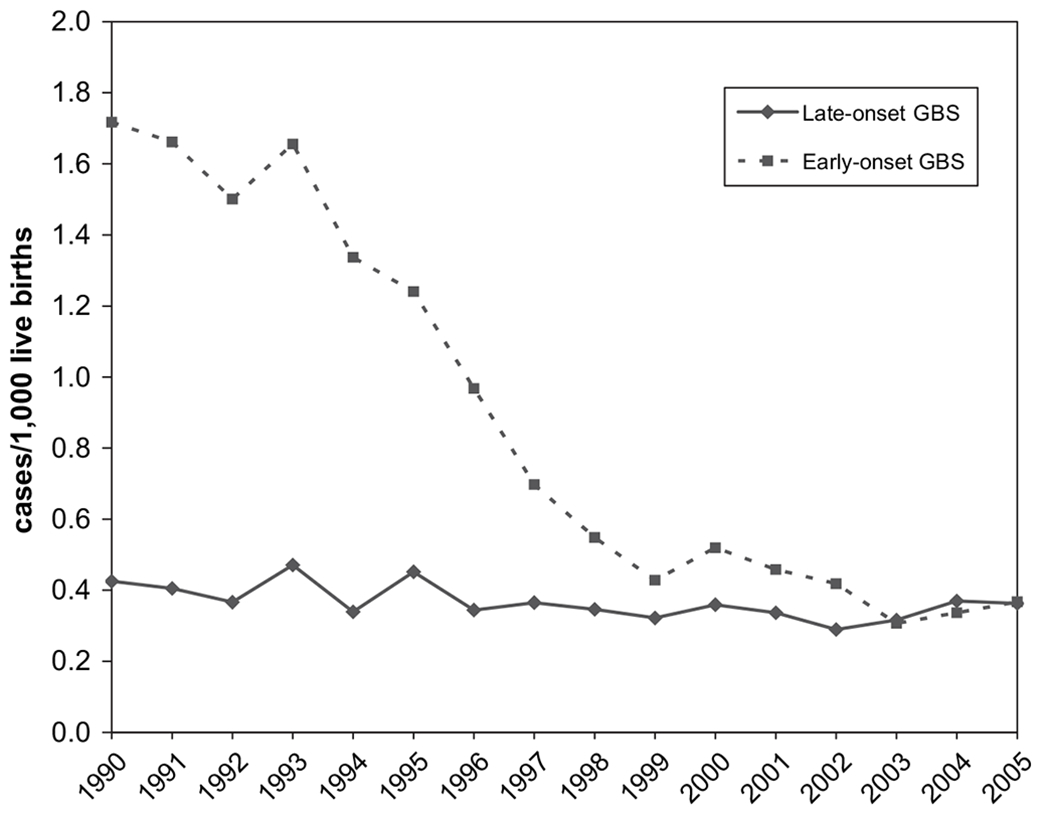
Trends in early- and late-onset neonatal group B streptococcal infections in active bacterial core surveillance areas, United States, 1990–2005. (Adapted from Jordan HT, Farley MM, Craig A, et al. Revisiting the need for vaccine prevention of late-onset neonatal group B streptococcal disease. Pediatr Infect Dis J 2008;27:1060; with permission.)
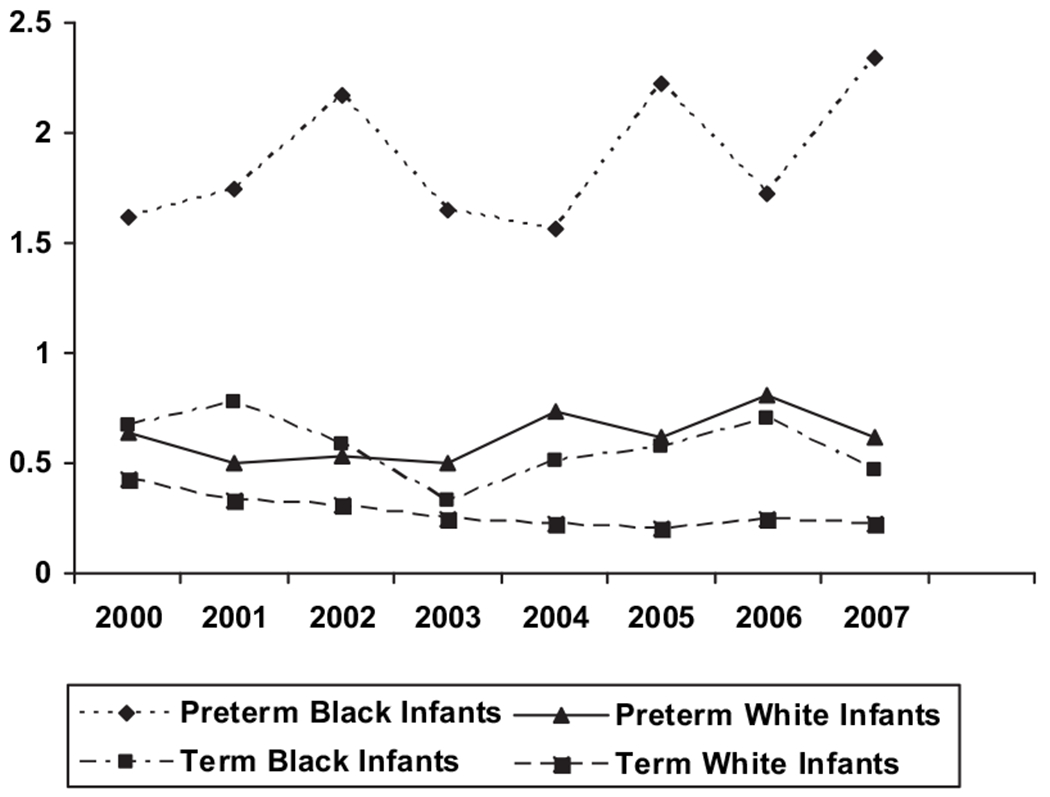
Early-onset group B streptococcal incidence rates in active bacterial core surveillance areas stratified by race and term, 2000—2007. (Adapted from CDC. Trends in perinatal group B streptococcal disease—United States, 2000–2006. MMWR Morb Mortal Wkly Rep 2009;58:109–12.)
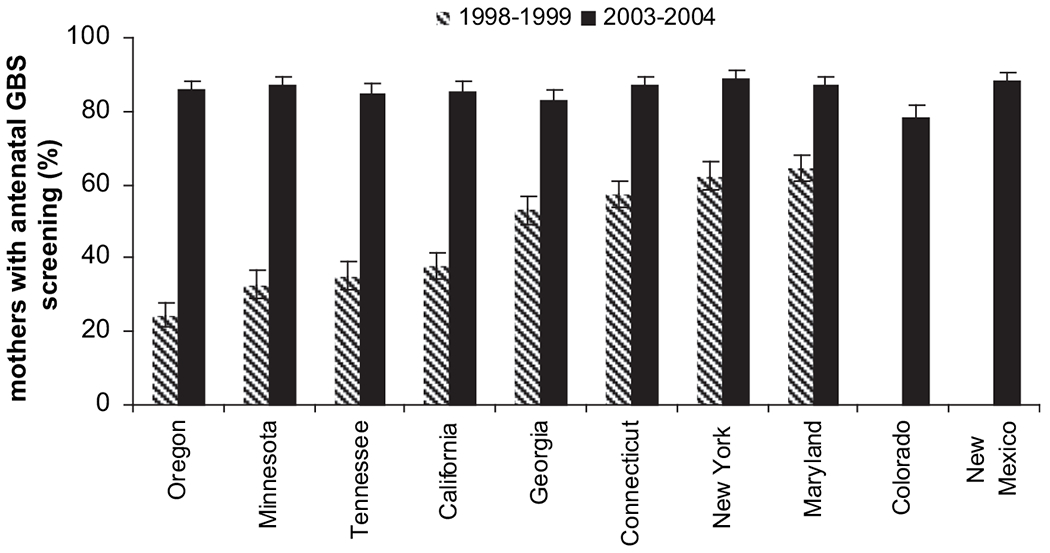
Proportion of pregnant women with antenatal screening for GBS in active bacterial core surveillance areas across the United States. (From Van Dyke MK, Phares CR, Lynfield R, et al. Evaluation of universal antenatal screening for Group B Streptococcus. NEJM 2009;360:2630; with permission.)
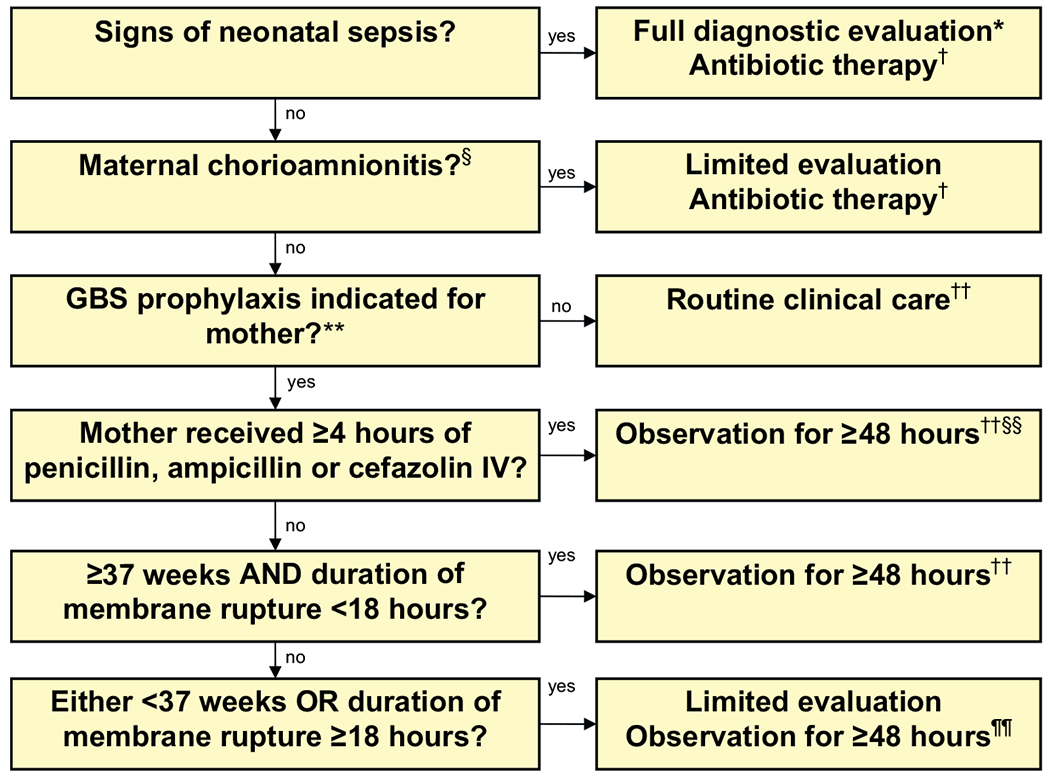
Algorithm for recommended management of newborns at risk for group B streptococcal disease. * Includes CBC with differential, platelets, blood culture, chest radiograph (if respiratory abnormalities are present), and LP (if patient stable enough to tolerate procedure and sepsis is suspected). † Antibiotic therapy should be directed towards the most common causes of neonatal sepsis including GBS and other organisms (including gram negative pathgoens), and should take into account local antibiotic resistance patterns. § Consultation with obstetric providers is important to determine the level of clinical suspicion for chorioamnionitis. Chorioamnionitis is diagnosed clinically and some of the signs are non-specific. ¶ Includes blood culture (at birth), and CBC with differential and platelets. Some experts recommend a CBC with differential and platelets at 6-12 hours of age. ** GBS prophylaxis indicated if one or more of the following: (1) mother GBS positive at 35-37 weeks’ gestation, (2) GBS status unknown with one or more intrapartum risk factors including <37 weeks’ gestation, ROM ≥ 18 hours or T ≥100.4°F (38.0°C), (3) GBS bacteriuria during current pregnancy, (4) history of a previous infant with GBS disease. †† If signs of sepsis develop, a full diagnostic evaluation should be done and antibiotic therapy initiated. §§ If ≥37 weeks’ gestation, observation may occur at home after 24 hours if there is a knowledgeable observer and ready access to medical care. ¶¶ Some experts recommend a CBC with differential and platelets at 6-12 hours of age.
References
-
- Baker CJ, Barrett FF, Gordon RC, et al. Suppurative meningitis due to streptococci of Lancefield group B: a study of 33 infants. J Pediatr 1973;82(4):724–9. - PubMed
-
- Barton LL, Feigin RD, Lins R. Group B beta hemolytic streptococcal meningitis in infants. J Pediatr 1973;82(4):719–23. - PubMed
-
- Franciosi RA, Knostman JD, Zimmerman RA. Group B streptococcal neonatal and infant infections. J Pediatr 1973;82(4):707–18. - PubMed
-
- CDC. Trends in perinatal group B streptococcal disease—United States, 2000–2006. MMWR Morb Mortal Wkly Rep 2009;58(5):109–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
