

Infection rate and acute organ dysfunction risk as explanations for racial differences in severe sepsis
- PMID: 20571016
- PMCID: PMC3910506
- DOI: 10.1001/jama.2010.851
Infection rate and acute organ dysfunction risk as explanations for racial differences in severe sepsis
Abstract
Context: Severe sepsis, defined as infection complicated by acute organ dysfunction, occurs more frequently and leads to more deaths in black than in white individuals. The optimal approach to minimize these disparities is unclear.
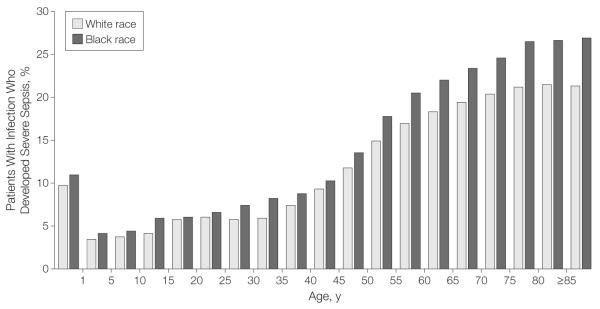
Objective: To determine the extent to which higher severe sepsis rates in black than in white patients are due to higher infection rates or to a higher risk of acute organ dysfunction.
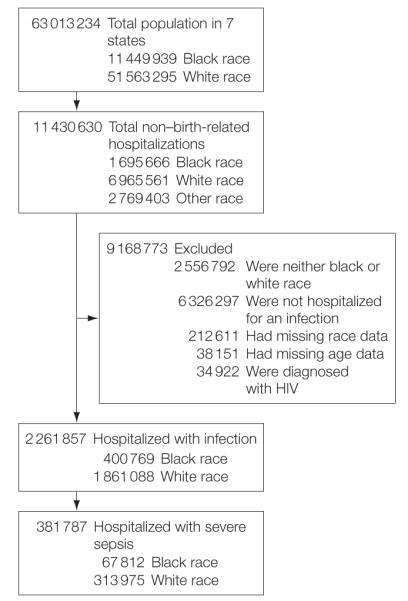
Design, setting, and participants: Analysis of infection-related hospitalizations from the 2005 hospital discharge data of 7 US states and infection-related emergency department visits from the 2003-2007 National Hospital Ambulatory Care Survey.
Main outcome measure: Age- and sex-standardized severe sepsis and infection hospitalization rates and the risk of acute organ dysfunction.
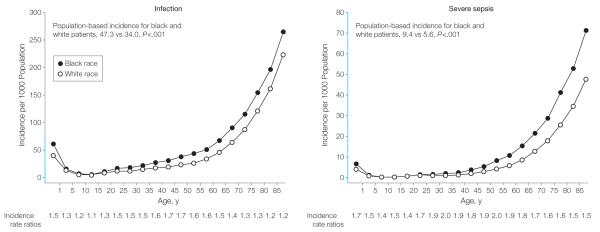
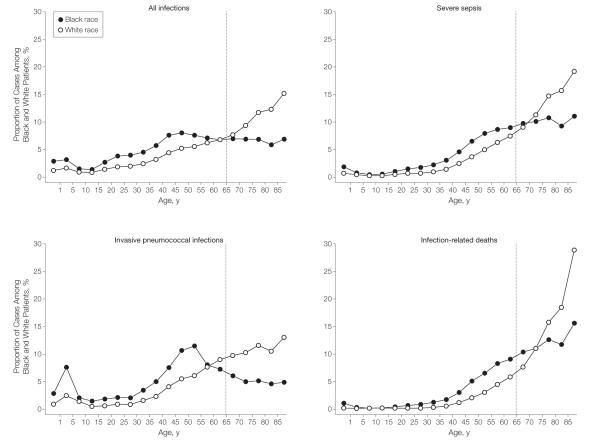
Results: Of 8,661,227 non-childbirth-related discharges, 2,261,857 were associated with an infection, and of these, 381,787 (16.8%) had severe sepsis. Black patients had a 67% higher age- and sex-standardized severe sepsis rate than did white patients (9.4; 95% confidence interval [CI], 9.3-9.5 vs 5.6; 95% CI, 5.6-5.6 per 1000 population; P < .001) and 80% higher standardized mortality (1.8, 95% CI, 1.8-1.9 vs 1.0, 95% CI, 1.0-1.1 per 1000 population; P < .001). The higher severe sepsis rate was explained by both a higher infection rate in black patients (47.3; 95% CI, 47.1-47.4 vs 34.0; 95% CI, 33.9-34.0 per 1000 population; incidence rate ratio, 1.39; P < .001) and a higher risk of developing acute organ dysfunction (age- and sex-adjusted odds ratio [OR], 1.29; 95% CI, 1.27-1.30; P < .001). Differences in infection presented broadly across different sites and etiology of infection and for community- and hospital-acquired infections and occurred despite a lower likelihood of being admitted for infection from the emergency department (adjusted OR, 0.70; 95% CI, 0.64-0.76; P < .001). The higher risk of organ dysfunction persisted but was attenuated after adjusting for age, sex, comorbid conditions, poverty, and hospital effect (OR, 1.14; 95% CI, 1.13-1.16; P < .001). Racial disparities in infection and severe sepsis incidence and mortality rates were largest among younger adults (eg, the proportion of invasive pneumococcal disease occurring in adults < 65 years was 73.9% among black patients vs 44.5% among white patients, P < .001).
Conclusion: Racial differences in severe sepsis are explained by both a higher infection rate and a higher risk of acute organ dysfunction in black than in white individuals.
Figures
Comment in
-
Racial differences in rates of severe sepsis.JAMA. 2010 Oct 13;304(14):1556; author reply 1556. doi: 10.1001/jama.2010.1441. JAMA. 2010. PMID: 20940380 No abstract available.
References
-
- Levy MM, Fink MP, Marshall JC, et al. SCCM/ESICM/ACCP/ATS/SIS.2001SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. CritCare Med. 2003;31(4):1250–1256. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–1310. - PubMed
-
- Laterre PF, Garber G, Levy H, et al. PROWESS Clinical Evaluation Committee. Severe community-acquired pneumonia as a cause of severe sepsis: data from the PROWESS study. Crit Care Med. 2005;33(5):952–961. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
