

Influence of patients' preferences and treatment site on cancer patients' end-of-life care
- PMID: 20572030
- PMCID: PMC3670423
- DOI: 10.1002/cncr.25217
Influence of patients' preferences and treatment site on cancer patients' end-of-life care
Abstract
Background: Research suggests that patients' end-of-life (EOL) care is determined primarily by the medical resources available, and not by patient preferences. The authors examined whether patients' desire for life-extending therapy was associated with their EOL care.
Methods: Coping with Cancer is a multisite, prospective, longitudinal study of patients with advanced cancer. Three hundred one patients were interviewed at baseline and followed until death, a median of 4.5 months later. Multivariate analyses examined the influence of patients' preferences and treatment site on whether patients received intensive care or hospice services in the final week of life.
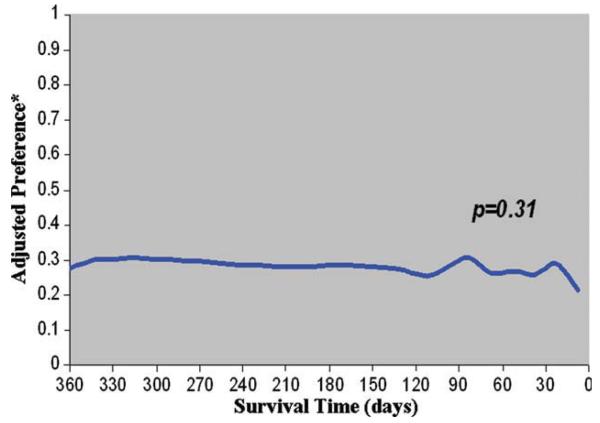
Results: Eighty-three of 301 patients (27.6%) with advanced cancer wanted life-extending therapy at baseline. Patients who understood that their disease was terminal or who reported having EOL discussions with their physicians were less likely to want life-extending care compared with others (23.4% vs 42.6% and 20.7% vs 44.4%, respectively; P≤.003). Patients who were treated at Yale Cancer Center received more intensive care (odds ratio [OR], 3.14; 95% confidence interval [CI], 1.16-8.47) and less hospice services (OR, 0.52; 95% CI, 0.29-0.92) compared with patients who were treated at Parkland Hospital. However, in multivariate analyses that controlled for confounding influences, patients who preferred life-extending care were more likely to receive intensive care (adjusted OR [AOR], 2.91; 95% CI, 1.09-7.72) and were less likely to receive hospice services (AOR, 0.45; 95% CI, 0.26-0.78). Treatment site was not identified as a significant predictor of EOL care.
Conclusions: The treatment preferences of patients with advanced cancer may play a more important role in determining the intensity of medical care received at the EOL than previously recognized. Future research is needed to determine the mechanisms by which patients' preferences for care and treatment site interact to influence EOL care.
Copyright © 2010 American Cancer Society.
Figures
Similar articles
-
Provision of spiritual support to patients with advanced cancer by religious communities and associations with medical care at the end of life.JAMA Intern Med. 2013 Jun 24;173(12):1109-17. doi: 10.1001/jamainternmed.2013.903. JAMA Intern Med. 2013. PMID: 23649656 Free PMC article.
-
Predictors of intensive end-of-life and hospice care in Latino and white advanced cancer patients.J Palliat Med. 2013 Oct;16(10):1249-54. doi: 10.1089/jpm.2013.0164. Epub 2013 Sep 20. J Palliat Med. 2013. PMID: 24053593 Free PMC article.
-
Minor cognitive impairments in cancer patients magnify the effect of caregiver preferences on end-of-life care.J Pain Symptom Manage. 2013 Apr;45(4):650-9. doi: 10.1016/j.jpainsymman.2012.03.003. Epub 2012 Jul 28. J Pain Symptom Manage. 2013. PMID: 22846621 Free PMC article. Clinical Trial.
-
Straddling the fence: ICU nurses advocating for hospice care.Crit Care Nurs Clin North Am. 2012 Mar;24(1):105-16. doi: 10.1016/j.ccell.2012.01.006. Crit Care Nurs Clin North Am. 2012. PMID: 22405716 Review.
-
Associations Among End-of-Life Discussions, Health-Care Utilization, and Costs in Persons With Advanced Cancer: A Systematic Review.Am J Hosp Palliat Care. 2019 Oct;36(10):913-926. doi: 10.1177/1049909119848148. Epub 2019 May 9. Am J Hosp Palliat Care. 2019. PMID: 31072109 Free PMC article.
Cited by
-
Accuracy of advanced cancer patients' life expectancy estimates: The role of race and source of life expectancy information.Cancer. 2016 Jun 15;122(12):1905-12. doi: 10.1002/cncr.30001. Epub 2016 Mar 29. Cancer. 2016. PMID: 27028270 Free PMC article.
-
Marginal treatment benefit in anaplastic thyroid cancer.Cancer. 2013 Sep 1;119(17):3133-9. doi: 10.1002/cncr.28187. Epub 2013 Jul 9. Cancer. 2013. PMID: 23839797 Free PMC article.
-
Prognosticating Outcomes and Nudging Decisions with Electronic Records in the Intensive Care Unit Trial Protocol.Ann Am Thorac Soc. 2021 Feb;18(2):336-346. doi: 10.1513/AnnalsATS.202002-088SD. Ann Am Thorac Soc. 2021. PMID: 32936675 Free PMC article.
-
Associations of prognostic-awareness-transition patterns with end-of-life care in cancer patients' last month.Support Care Cancer. 2022 Jul;30(7):5975-5989. doi: 10.1007/s00520-022-07007-4. Epub 2022 Apr 8. Support Care Cancer. 2022. PMID: 35391576
-
Prospective Comparison of Medical Oncologists and a Machine Learning Model to Predict 3-Month Mortality in Patients With Metastatic Solid Tumors.JAMA Netw Open. 2022 May 2;5(5):e2214514. doi: 10.1001/jamanetworkopen.2022.14514. JAMA Netw Open. 2022. PMID: 35639380 Free PMC article.
References
-
- Wennberg JE, Freeman JL, Shelton RM, et al. Hospital use and mortality among Medicare beneficiaries in Boston and New Haven. N Engl J Med. 1989;321:1168–1173. - PubMed
-
- Danis M, Mutran E, Garrett JM, et al. A prospective study of the impact of patient preferences on life-sustaining treatment and hospital cost. Crit Care Med. 1996;24:1811–1817. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
