

Increased neck soft tissue mass and worsening of obstructive sleep apnea after growth hormone treatment in men with abdominal obesity
- PMID: 20572419
- PMCID: PMC2883037
Increased neck soft tissue mass and worsening of obstructive sleep apnea after growth hormone treatment in men with abdominal obesity
Abstract
Background: Risk factors for obstructive sleep apnea (OSA) are male gender, obesity and abnormalities in neck soft tissue mass. OSA is associated with both growth hormone (GH) excess and severe GH deficiency in adults. Adults with abdominal obesity have markedly suppressed GH secretion.
Aim: To study the effect of GH treatment on OSA in abdominally obese men with impaired glucose tolerance.
Patients and methods: Forty men with abdominal obesity and glucose intolerance were randomized in a prospective, 12-month double-blind trial to receive either GH or placebo. The treatment groups had similar BMI and waist circumference. Overnight polysomnography and computed tomography to assess muscle and fat distribution in the neck and abdomen were performed at baseline and after 12 months.
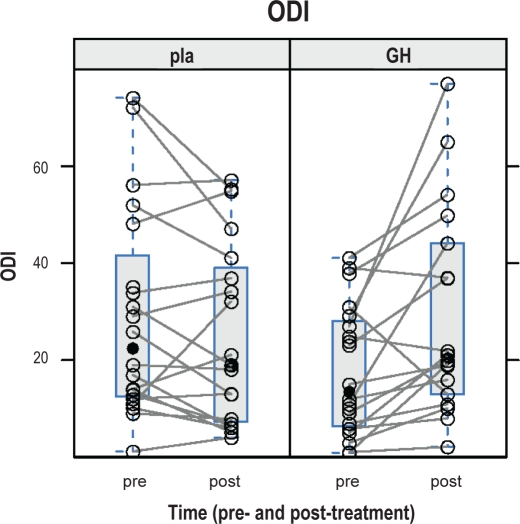
Results: GH treatment increased insulin-like growth-factor-1i from (mean [SD]) 168 (72) to 292 (117) microg/L, the apnea-hypopnea index from (n/h) 31 (20) to 43 (25) and oxygen-desaturation index from (n/h) 18 (14) to 29 (21) (p = 0.0001, 0.001, 0.002). Neck transverse diameter, circumference and total cross-sectional area (p = 0.007, 0.01, 0.02) increased, while abdominal visceral adipose tissue (p = 0.007) was reduced. No between-group differences in total sleep time, REM sleep, NREM sleep, and time spent in supine position were found. The Epworth sleepiness scale score was unchanged.
Conclusions: GH treatment increased the severity of OSA in abdominally obese men. The possible mechanism appears to be reflected by the GH-induced increase of measures of neck volume. The present results, to some extent, argue against that low GH/IGF-I activity is a primary cause of OSA in abdominally obese men.
Figures



References
-
- Coughlin SR, Mawdsley L, Mugarza JA, Calverley PM, Wilding JP. Obstructive sleep apnoea is independently associated with an increased prevalence of metabolic syndrome. Eur Heart J. 2004;25:735–41. - PubMed
-
- Dostalova S, Sonka K, Smahel Z, Weiss V, Marek J, Horinek D. Craniofacial abnormalities and their relevance for sleep apnoea syndrome aetiopathogenesis in acromegaly. Eur J Endocrinol. 2001;144:491–7. - PubMed
-
- Colao A, Ferone D, Marzullo P, Lombardi G. Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr Rev. 2004;25:102–52. - PubMed
-
- Hochban W, Ehlenz K, Conradt R, Brandenburg U. Obstructive sleep apnoea in acromegaly: the role of craniofacial changes. Eur Respir J. 1999;14:196–202. - PubMed
-
- Veldhuis JD, Iranmanesh A, Ho KK, Waters MJ, Johnson ML, Lizarralde G. Dual defects in pulsatile growth hormone secretion and clearance subserve the hyposomatotropism of obesity in man. J Clin Endocrinol Metab. 1991;72:51–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources