

Review
doi: 10.1056/NEJMcp1000274.
Clinical practice. Endometriosis
Affiliations
- PMID: 20573927
- PMCID: PMC3108065
- DOI: 10.1056/NEJMcp1000274
Item in Clipboard
Review
Clinical practice. Endometriosis
N Engl J Med.
.
Abstract
A healthy 25-year-old woman presents with worsening dysmenorrhea, pain of recent onset in the left lower quadrant, and dyspareunia. She has regular menstrual cycles, and her last menstrual period was 3 weeks before presentation. How should this patient be evaluated and treated?
Figures
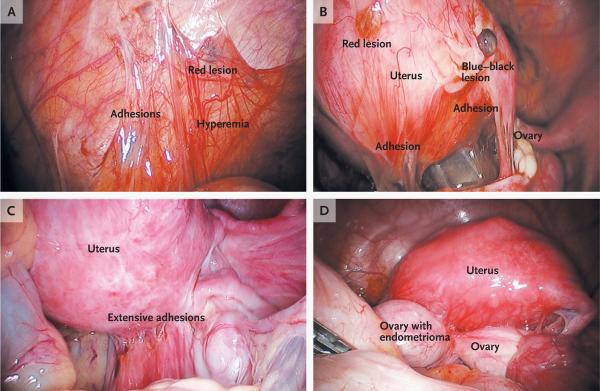
Panel A shows an endometriotic implant (red lesion), adhesions, and hyperemia in the peritoneum. Panel B shows peritoneal implants, including red and blue–black lesions and adhesions. Panel C shows extensive adhesions distorting the normal pelvic anatomy. Panel D shows an endometrioma adherent to the posterior uterus and distending the ovarian capsule. At surgery, it is difficult to distinguish visually an endometrioma from a cyst of the corpus luteum, a hemorrhagic cyst, or a simple cyst. Although the cyst fluid in endometriomas is thick and dark brown because it contains hemosiderin (hence, the name “chocolate cysts”), this color is not specific to endometriomas. (Images courtesy of Dr. Christopher Herndon, University of California, San Francisco.)
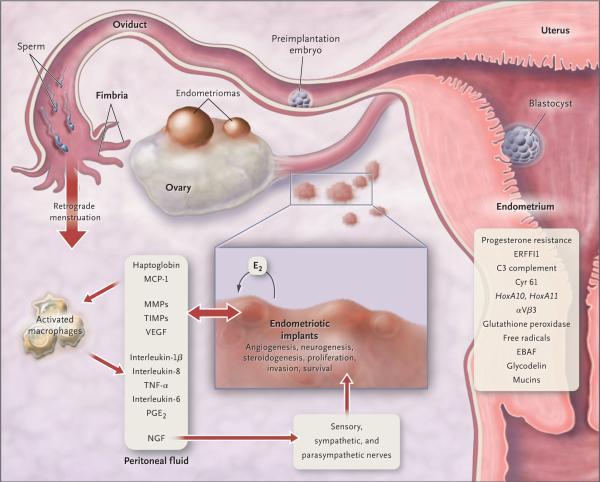
Retrograde transplanted endometrial tissue and cells attach to peritoneal surfaces, establish a blood supply, and invade nearby structures. They are infiltrated by sensory, sympathetic, and parasympathetic nerves and elicit an inflammatory response. Endometriotic implants secrete estradiol (E2) as well as prostaglandin E2 (PGE2), agents that attract macrophages (monocyte chemotactic protein 1 [MCP-1]), neurotrophic peptides (nerve growth factor [NGF]), enzymes for tissue remodeling (matrix metalloproteinases [MMPs]) and tissue inhibitors of MMPs (TIMPs), and proangiogenic substances such as vascular endothelial growth factor (VEGF) and interleukin-8. Lesions secrete haptoglobin, which decreases macrophage adhesion and phagocytic function. Lesions and activated macrophages, which are abundant in the peritoneal fluid in women with endometriosis, also secrete proinflammatory cytokines (interleukin-1β, interleukin-8, interleukin-6, and tumor necrosis factor α [TNF-α]). Local (and systemic) estradiol can stimulate lesion production of PGE2, which can activate pain fibers, enhance neuronal invasion of lesions by stimulating production of NGF and other neurotrophins, and promote sprouting of nociceptors that contribute to persistent inflammatory pain and inhibit neuronal apoptosis. Endometrial bleeding factor (EBAF) is misexpressed and may contribute to uterine bleeding. Infertility results from the toxic effects of the inflammatory process on gametes and embryos, compromised fimbrial function, and eutopic endometrium that is resistant to the action of progesterone and is inhospitable to embryonic implantation. HoxA10 and HoxA11 genes and αVβ3 integrin are not up-regulated by progesterone, and thus the endometrium is inhospitable to an implanting embryo. Endocrine-disrupting chemicals can contribute to progesterone resistance and perhaps immune dysfunction., ERFFI1 (ErbB receptor feedback inhibitor 1) is constitutively expressed and there is excess mitogenic signaling.
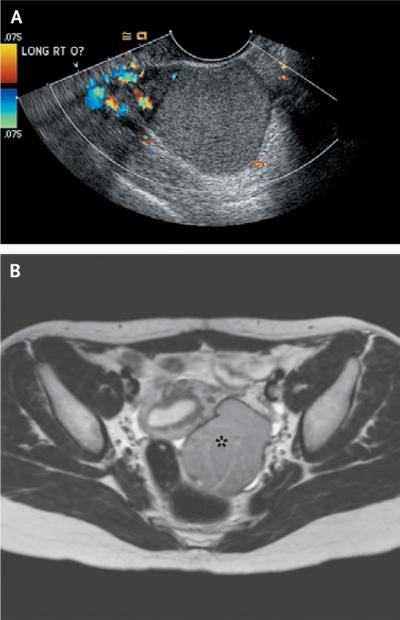
The transvaginal ultrasonogram in Panel A shows the ground-glass appearance of a 5-cm right ovarian endometrioma, with little flow to the mass but normal flow to the ovary. The red, yellow, and orange areas indicate blood flow toward the transducer, and the blue and green areas indicate blood flow away from the transducer. The T2-weighted magnetic resonance image in Panel B shows a left ovarian endometrioma (asterisk). (Images courtesy of Dr. Christopher Herndon, University of California, San Francisco.)
References
-
- Giudice LC, Swiersz RO. LM, Burney Endometriosis. In: Jameson JL, De Groot LJ, editors. Endocrinology. 6th ed. Elsevier; New York: 2010. pp. 2356–70.
-
- Goldstein DP, deCholnoky C, Emans SJ, Leventhal JM. Laparoscopy in the diagnosis and management of pelvic pain in adolescents. J Reprod Med. 1980;24:251–6. - PubMed
-
- Eskenazi B, Warner ML. Epidemiology of endometriosis. Obstet Gynecol Clin North Am. 1997;24:235–58. - PubMed
-
- Bulun SE. Endometriosis. N Engl J Med. 2009;360:268–79. - PubMed
-
- Berkley KJ, Rapkin AJ, Papka RE. The pains of endometriosis. Science. 2005;308:1587–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical