

Ovine surgical model of uterine space restriction: interactive effects of uterine anomalies and multifetal gestations on fetal and placental growth
- PMID: 20574052
- PMCID: PMC2959109
- DOI: 10.1095/biolreprod.110.085381
Ovine surgical model of uterine space restriction: interactive effects of uterine anomalies and multifetal gestations on fetal and placental growth
Abstract
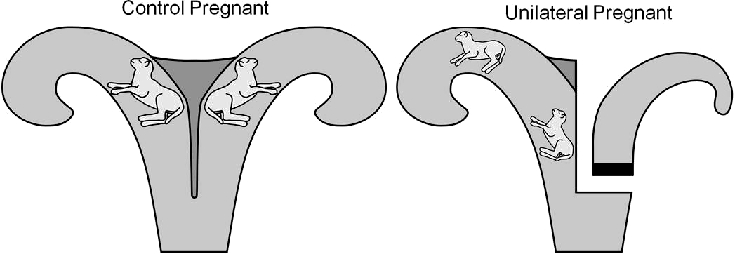
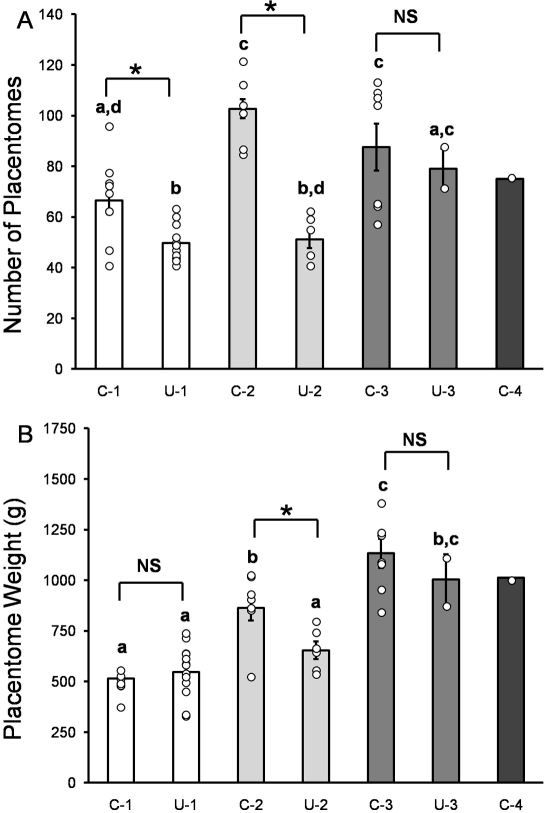
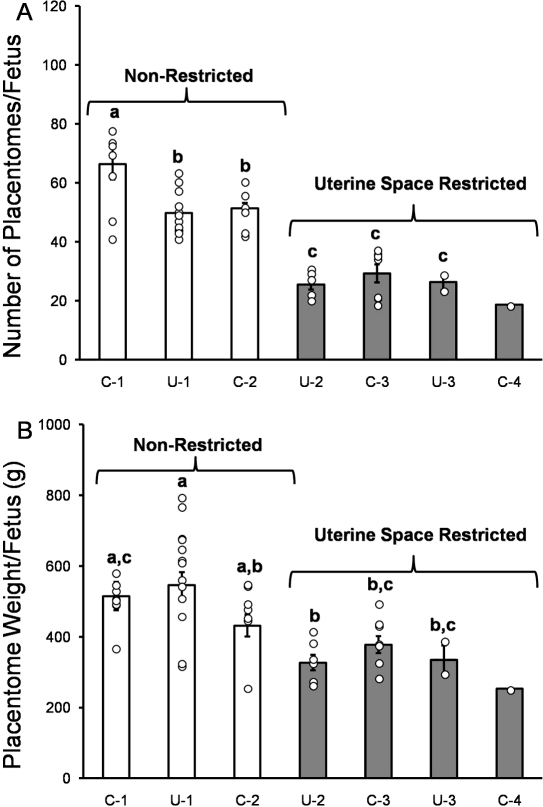
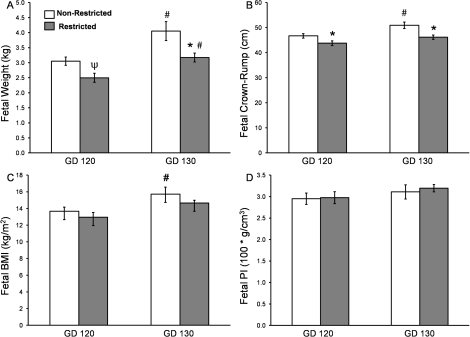
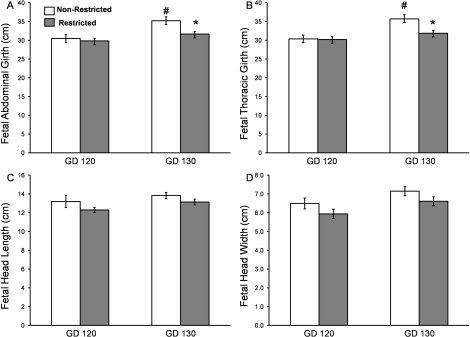
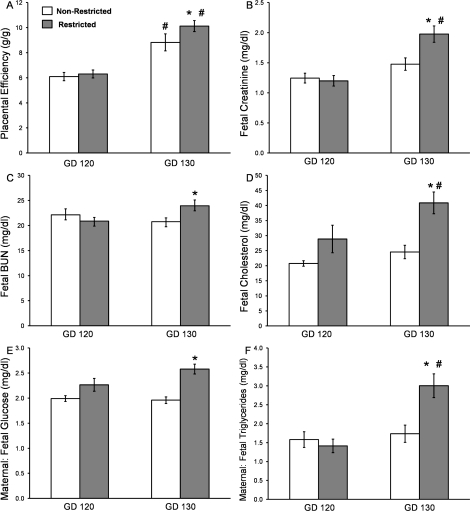
Intrauterine growth restriction (IUGR) is observed in conditions with limitations in uterine space (e.g., uterine anomalies and multifetal gestations). IUGR is associated with reduced fetal weight, organ growth, and a spectrum of adult-onset diseases. To examine the interaction of uterine anomalies and multifetal gestations, we developed a surgical uterine space restriction model with a unilateral uterine horn ligation before breeding (unilateral surgery). Placentas and fetuses were studied on Gestational Day (GD) 120 and GD 130 (term = 147 days). Unilateral surgery decreased placentome numbers in singleton and twin pregnancies (25% and 50%, respectively) but not unilateral triplets. Unilateral surgery decreased total placentome weight in twin pregnancies (decreased 24%). Fetuses categorized as uterine space restricted (unilateral twin and both groups of triplets) had 51% fewer placentomes per fetus and a 31% reduction in placentomal weight per fetus compared to the nonrestricted group (control singleton, unilateral singleton, and control twin). By GD 130, uterine space-restricted fetuses exhibited decreased weight, smaller crown-rump, abdominal girth, and thoracic girth as well as decreased fetal heart, kidney, liver, spleen, and thymus weights. Lung and brain weights were unaffected, demonstrating asymmetric IUGR. At GD 130, placental efficiency (fetal weight per total placentomal weight) was elevated in uterine space-restricted fetuses. However, fetal arterial creatinine, blood urea nitrogen, and cholesterol were elevated, suggesting insufficient placental clearance. Maternal-to-fetal glucose and triglycerides ratios were elevated in the uterine space-restricted pregnancies, suggesting placental nutrient transport insufficiency. This model allows for examination of interactive effects of uterine space restriction-induced IUGR on placental adaptation and fetal organ growth.
Figures
References
-
- Grimbizis GF, Camus M, Tarlatzis BC, Bontis JN, Devroey P.Clinical implications of uterine malformations and hysteroscopic treatment results. Hum Reprod Update 2001; 7: 161–174. - PubMed
-
- Kiely JL, Brett KM, Yu S, Rowley D.Low birth weight and intrauterine growth retardation. Wilcox LS, Marks JS.From Data To Action: CDC's Public Health Surveillance For Women, Infants, And Children. Washington, DC: US Department of Health and Human Services; 1994: 185–202.
-
- Romo A, Carceller R, Tobajas J.Intrauterine growth retardation (IUGR): epidemiology and etiology. Pediatr Endocrinol Rev 2009; 6(suppl 3):332–336. - PubMed
-
- Reichman D, Laufer MR, Robinson BK.Pregnancy outcomes in unicornuate uteri: a review. Fertil Steril 2009; 91: 1886–1894. - PubMed
-
- Cohen A, Chhibber G.Obstetric complications of congenital anomalies of the paramesonephric ducts. Semin Reprod Endocrinol 1986; 4: 59–65.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
