

Reconstruction of the breast conservation deformity
- PMID: 20574487
- PMCID: PMC2884729
- DOI: 10.1055/s-2004-829043
Reconstruction of the breast conservation deformity
Abstract
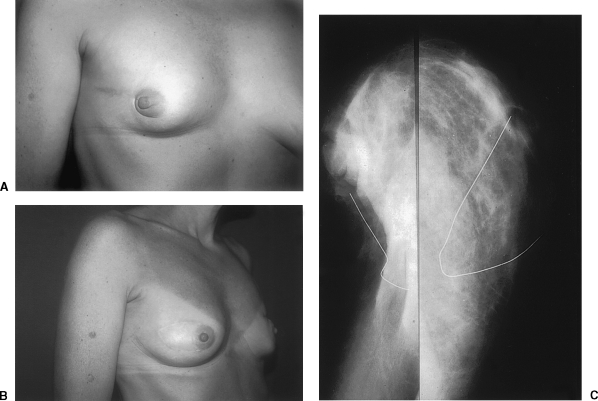
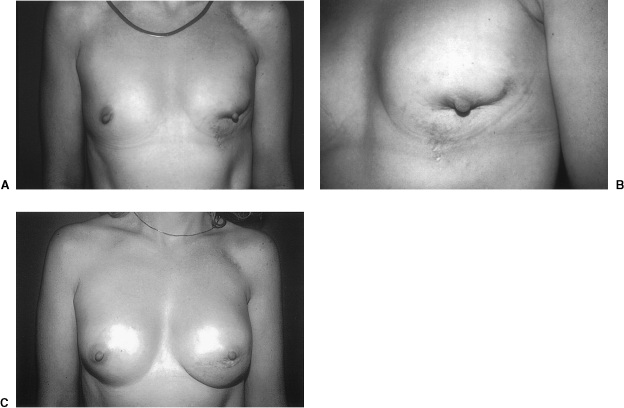
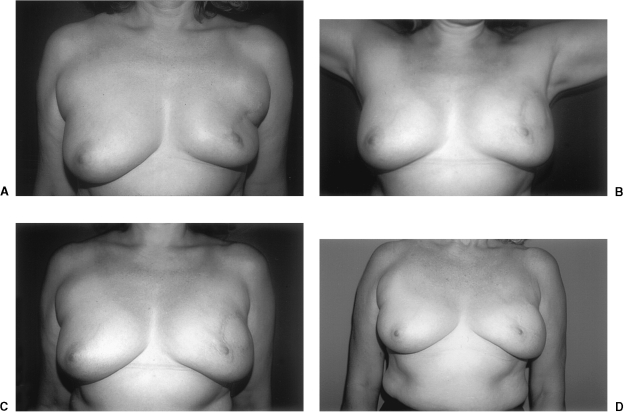
The era of breast conserving treatment of early-stage breast carcinoma has created reconstructive challenges for the plastic surgeon. Although good to excellent cosmetic outcomes occur in the majority of patients, a significant number could benefit from additional reconstructive measures. Because of the need for continuing surveillance following breast-conserving therapy, estimated at 5-10% after fifteen years, plastic surgeons should choose techniques that do not interfere with the detection of recurrent breast carcinoma. Myocutaneous flaps-in particular, the latissimus dorsi and transverse rectus abdominis-have fulfilled the reconstructive needs of these patients by providing well-vascularized soft tissue. Postoperative radiological evaluation has demonstrated that these flaps are radiolucent, unlike breast implants that can obscure accurate mammographic interpretation.Myocutaneous flaps have been used for both immediate and delayed reconstruction of post-breast conservation deformities. The delayed approach offers the benefit of an established contour deformity that usually involves cutaneous, parenchymal, and nipple-areolar components. Moderate overcorrection of the defect has been advocated in anticipation of ongoing postradiation wound contraction and fibrosis. Immediate reconstruction of lumpectomy and partial mastectomy defects permits wider initial excision of the breast lesion, but can be compromised by positive histological margins. Long-term results suggest stability of the aesthetic outcome following reconstruction of delayed deformities.
Keywords: Reconstruction; breast; conservation; deformity.
Figures

Similar articles
-
Reconstruction of the radiated partial mastectomy defect with autogenous tissues.Plast Reconstr Surg. 1992 Nov;90(5):854-65; discussion 866-9. Plast Reconstr Surg. 1992. PMID: 1410039
-
Recurrent breast cancer following immediate reconstruction with myocutaneous flaps.Plast Reconstr Surg. 1994 May;93(6):1191-204; discussion 1205-7. doi: 10.1097/00006534-199405000-00013. Plast Reconstr Surg. 1994. PMID: 8171139
-
Skin- and Nipple-Areola-Sparing Mastectomy with Immediate Breast Reconstruction Using Transverse Rectus Abdominis Myocutaneous Flap and Silicone Implants in Breast Carcinoma Patients.Oncol Res Treat. 2020;43(7-8):354-361. doi: 10.1159/000506841. Epub 2020 Jun 22. Oncol Res Treat. 2020. PMID: 32570247
-
Breast reconstructive techniques in cancer patients: which ones, when to apply, which immediate and long term risks?Crit Rev Oncol Hematol. 2001 Jun;38(3):231-9. doi: 10.1016/s1040-8428(00)00137-2. Crit Rev Oncol Hematol. 2001. PMID: 11369256 Review.
-
Advances in breast reconstruction after mastectomy.J Long Term Eff Med Implants. 2005;15(2):197-207. doi: 10.1615/jlongtermeffmedimplants.v15.i2.70. J Long Term Eff Med Implants. 2005. PMID: 15777171 Review.
Cited by
-
Usefulness of a lateral thoracodorsal flap after breast conserving surgery in laterally located breast cancer.Arch Plast Surg. 2013 Jul;40(4):367-73. doi: 10.5999/aps.2013.40.4.367. Epub 2013 Jul 17. Arch Plast Surg. 2013. PMID: 23898433 Free PMC article.
-
Current aspects of therapeutic reduction mammaplasty for immediate early breast cancer management: An update.World J Clin Oncol. 2014 Feb 10;5(1):1-18. doi: 10.5306/wjco.v5.i1.1. World J Clin Oncol. 2014. PMID: 24527398 Free PMC article. Review.
-
Use of a Bioabsorbable Implant-Acellular Dermal Matrix Construct to Facilitate Oncoplastic Breast-conserving Surgery.Plast Reconstr Surg Glob Open. 2021 Jan 25;9(1):e3356. doi: 10.1097/GOX.0000000000003356. eCollection 2021 Jan. Plast Reconstr Surg Glob Open. 2021. PMID: 33564586 Free PMC article.
-
Recognizing and Managing Breast Implant Complications: A Review for Healthcare Providers Who Treat Women Who Underwent Breast Implant-Based Surgery.Int J Womens Health. 2025 May 7;17:1297-1312. doi: 10.2147/IJWH.S501800. eCollection 2025. Int J Womens Health. 2025. PMID: 40357021 Free PMC article. Review.
-
Anterior intercostal artery perforator flap for immediate reconstruction following breast conservation surgery.Microsurgery. 2023 Jan;43(1):20-26. doi: 10.1002/micr.30884. Epub 2022 Mar 21. Microsurgery. 2023. PMID: 35312091 Free PMC article.
References
-
- Fisher B, Redmond C, Fisher E R, et al. Ten-year results of a randomized clinical trial comparing radical mastectomy and total mastectomy with or without radiation. N Engl J Med. 1985;312:674–681. - PubMed
-
- Jacobson J A, Danforth D N, Cowan K H, et al. Ten-year results of a comparison of conservation with mastectomy in the treatment of stage I and II breast cancer. N Engl J Med. 1995;332:907–911. - PubMed
-
- Veronesi U, Banfi A, Delvecchio M, et al. Comparison of Halsted mastectomy with quadrantectomy, axillary dissection and radiotherapy in early breast cancer: long term results. Eur J Cancer Clin Oncol. 1986;22:1085–1089. - PubMed
-
- Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347:1227–1232. - PubMed
