

Chest wall reconstruction and advanced disease
- PMID: 20574490
- PMCID: PMC2884721
- DOI: 10.1055/s-2004-829046
Chest wall reconstruction and advanced disease
Abstract
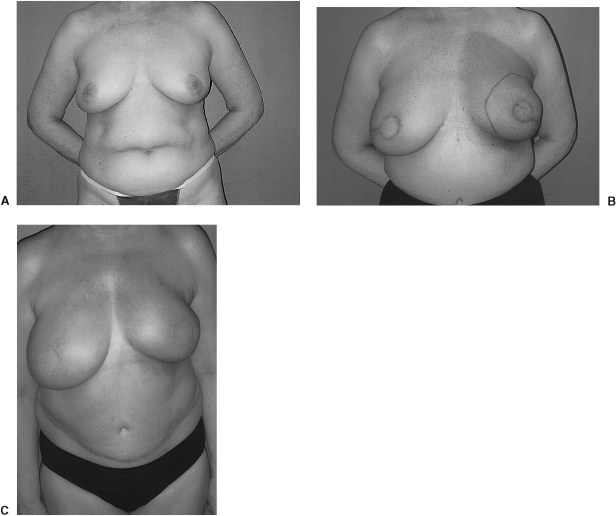
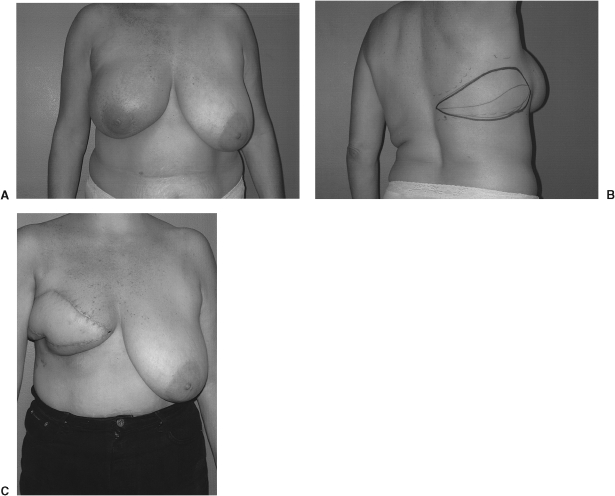
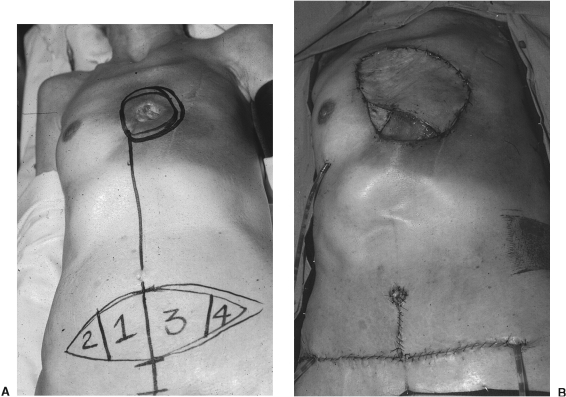
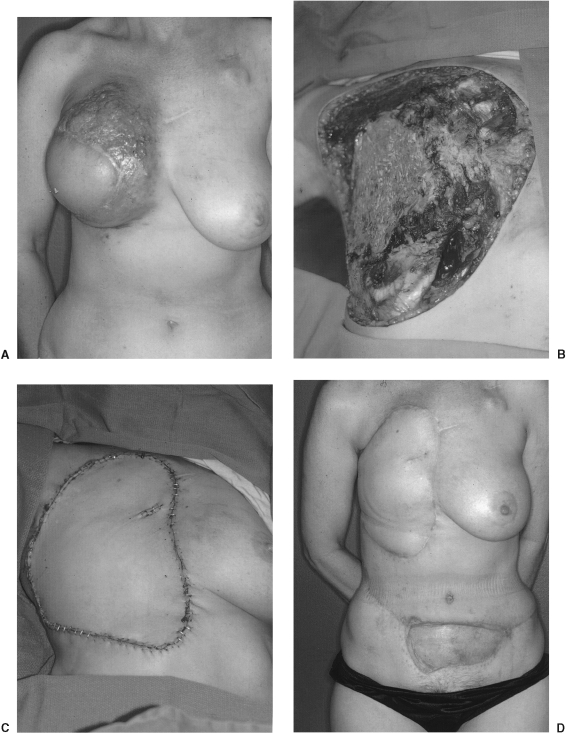
Clinical experience supports a role for palliative procedures in patients with locally advanced or recurrent breast cancer, yet numerous challenges are entailed in both the extirpation and reconstruction of the chest wall in these cases. The defects may be profound and complicated by prior surgery, radiation therapy, or patient-related variables. The reconstructive techniques employed must neither encumber nor delay any necessary postoperative therapy and must not result in unacceptable morbidity or compromise quality of life. Our surgical approach to these cases incorporates a team of specialists from a broad spectrum of medical and surgical disciplines. Each operative plan is tailored to the specific needs and requirements of the individual patient.
Keywords: Chest wall reconstruction; advanced breast cancer.
Figures


Similar articles
-
Thoracic Wall Reconstruction after Tumor Resection.Front Oncol. 2015 Oct 29;5:247. doi: 10.3389/fonc.2015.00247. eCollection 2015. Front Oncol. 2015. PMID: 26579499 Free PMC article. Review.
-
[Significance of multidisplinary surgery in chest wall resection and reconstruction for selected patients with breast cancer].Zhonghua Zhong Liu Za Zhi. 2006 Nov;28(11):856-9. Zhonghua Zhong Liu Za Zhi. 2006. PMID: 17416011 Chinese.
-
Extensive Microsurgical Reconstruction of Chest Wall Defects for Locally Advanced Breast Cancer: A 10-Year Single-Unit Experience.Ann Plast Surg. 2020 Mar;84(3):293-299. doi: 10.1097/SAP.0000000000002000. Ann Plast Surg. 2020. PMID: 31335462
-
Microsurgical Reconstruction of Large Oncologic Chest Wall Defects for Locally Advanced Breast Cancer or Osteoradionecrosis: A Retrospective Review of 26 Cases over a 5-Year Period.J Reconstr Microsurg. 2016 Feb;32(2):121-7. doi: 10.1055/s-0035-1563395. Epub 2015 Aug 31. J Reconstr Microsurg. 2016. PMID: 26322490
-
Review of Procedures for Reconstruction of Soft Tissue Chest Wall Defects Following Advanced Breast Malignancies.Cancer Control. 2019 Jan-Dec;26(1):1073274819827284. doi: 10.1177/1073274819827284. Cancer Control. 2019. PMID: 30808195 Free PMC article. Review.
Cited by
-
Thoracic Wall Reconstruction after Tumor Resection.Front Oncol. 2015 Oct 29;5:247. doi: 10.3389/fonc.2015.00247. eCollection 2015. Front Oncol. 2015. PMID: 26579499 Free PMC article. Review.
-
Hyperbaric oxygen therapy for a refractory skin ulcer after radical mastectomy and radiation therapy: a case report.J Med Case Rep. 2017 Jan 4;11(1):5. doi: 10.1186/s13256-016-1168-0. J Med Case Rep. 2017. PMID: 28049509 Free PMC article.
-
Vertical Rectus Abdominis Myocutaneous Flap for Reconstruction of Forequarter Amputation Defect after Shoulder Soft Tissue Sarcoma Resection: Technical Consideration.Plast Reconstr Surg Glob Open. 2023 Jun 19;11(6):e5077. doi: 10.1097/GOX.0000000000005077. eCollection 2023 Jun. Plast Reconstr Surg Glob Open. 2023. PMID: 37342308 Free PMC article.
-
Reconstruction of chest wall chondrosarcoma with an anterolateral thigh free flap: An illustration of decision-making in chest wall reconstruction.Int J Surg Case Rep. 2013;4(8):669-74. doi: 10.1016/j.ijscr.2013.05.003. Epub 2013 May 16. Int J Surg Case Rep. 2013. PMID: 23849801 Free PMC article.
-
Chest wall reconstruction with a latissimus dorsi musculocutaneous flap via the pleural cavity.Interact Cardiovasc Thorac Surg. 2012 Jan;14(1):96-8. doi: 10.1093/icvts/ivr006. Epub 2011 Nov 15. Interact Cardiovasc Thorac Surg. 2012. PMID: 22108922 Free PMC article.
References
-
- Rudolph R, Vande B J, Schneider J A, et al. Slowed growth of cultured fibroblasts from human radiation wounds. Plast Reconstr Surg. 1988;82:669–677. - PubMed
-
- Hopewell J W, Calvo W, Jaenke R, et al. Microvasculature and radiation damage. Recent Results Cancer Res. 1993;130:1–16. - PubMed
-
- Chuang V P. Radiation-induced arthritis. Semin Roentgenol. 1994;29:64–69. - PubMed
-
- Mansfield C. Effects of radiation therapy on wound healing after mastectomy. Clin Plast Surg. 1979;6:19–26. - PubMed
-
- Huang E, Perkins G, McNeese M D, et al. Locoregional treatment outcomes for inoperable anthracycline-resistant breast cancer. Int J Radiat Oncol Biol Physiol. 2002;53:1225–1233. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
