

Humanized anti-interleukin-6-receptor antibody (tocilizumab) monotherapy is more effective in slowing radiographic progression in patients with rheumatoid arthritis at high baseline risk for structural damage evaluated with levels of biomarkers, radiography, and BMI: data from the SAMURAI study
- PMID: 20574648
- PMCID: PMC3036807
- DOI: 10.1007/s10165-010-0325-3
Humanized anti-interleukin-6-receptor antibody (tocilizumab) monotherapy is more effective in slowing radiographic progression in patients with rheumatoid arthritis at high baseline risk for structural damage evaluated with levels of biomarkers, radiography, and BMI: data from the SAMURAI study
Abstract
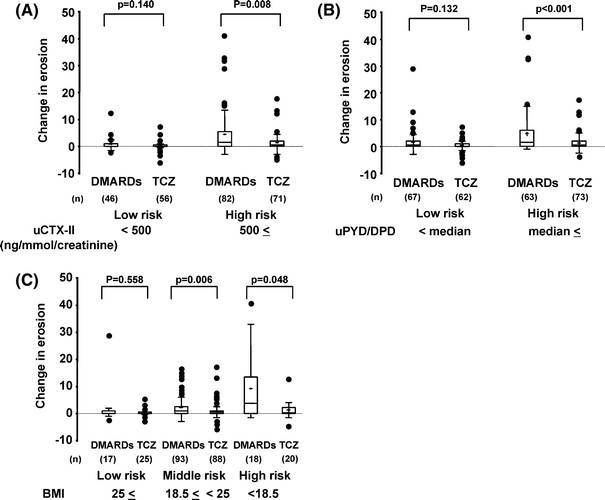
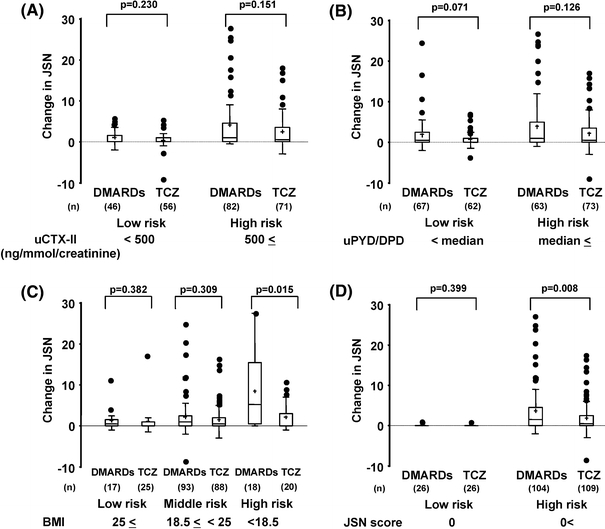
Our aim was to assess the ability of tocilizumab monotherapy to reduce progressive structural joint damage in rheumatoid arthritis patients at high risk of progression. This study was a subanalysis from a prospective 1-year, multicenter, X-ray-reader-blinded, randomized controlled trial of tocilizumab [Study of Active Controlled Monotherapy Used for Rheumatoid Arthritis, an IL-6 Inhibitor (SAMURAI) trial]. All patients were categorized into two or three groups according to four independent predictive markers for progressive joint damage [urinary C-terminal crosslinking telopeptide (uCTX-II), urinary pyridinoline/deoxypyridinoline (uPYD/DPD) ratio, body mass index (BMI), and joint-space narrowing (JSN) score at baseline]. One-year progression of joint destruction was assessed in high-risk versus low-risk groups receiving tocilizumab monotherapy and compared with patients receiving conventional disease-modifying antirheumatic drugs (DMARDs) (n = 157 and 145, respectively). In patients at high risk of progression of erosion as estimated by high uCTX-II, uPYD/DPD, or low BMI, and at high risk of progression of JSN as estimated by low BMI or high JSN score, the 52-week changes in radiological erosion and JSN, respectively, were significantly less in patients treated with tocilizumab monotherapy compared with those receiving DMARDs for each type of risk factor. In patients at low risk, those receiving tocilizumab also progressed less than those on DMARDs, although the difference did not reach statistical significance. Tocilizumab monotherapy is more effective in reducing radiological progression in patients presenting with risk factors for rapid progression than in low-risk patients. Patients at high risk for progression may benefit more from tocilizumab treatment.
Figures
Similar articles
-
A combination of biochemical markers of cartilage and bone turnover, radiographic damage and body mass index to predict the progression of joint destruction in patients with rheumatoid arthritis treated with disease-modifying anti-rheumatic drugs.Mod Rheumatol. 2009;19(3):273-82. doi: 10.1007/s10165-009-0170-4. Epub 2009 May 19. Mod Rheumatol. 2009. PMID: 19452245 Clinical Trial.
-
Study of active controlled monotherapy used for rheumatoid arthritis, an IL-6 inhibitor (SAMURAI): evidence of clinical and radiographic benefit from an x ray reader-blinded randomised controlled trial of tocilizumab.Ann Rheum Dis. 2007 Sep;66(9):1162-7. doi: 10.1136/ard.2006.068064. Epub 2007 May 7. Ann Rheum Dis. 2007. PMID: 17485422 Free PMC article. Clinical Trial.
-
Tocilizumab inhibits progression of joint damage in rheumatoid arthritis irrespective of its anti-inflammatory effects: disassociation of the link between inflammation and destruction.Ann Rheum Dis. 2012 May;71(5):687-93. doi: 10.1136/annrheumdis-2011-200395. Epub 2011 Nov 25. Ann Rheum Dis. 2012. PMID: 22121130 Free PMC article. Clinical Trial.
-
Tocilizumab: a review of its use in the management of rheumatoid arthritis.Drugs. 2009;69(5):609-32. doi: 10.2165/00003495-200969050-00007. Drugs. 2009. PMID: 19368420 Review.
-
Intravenous tocilizumab: a review of its use in adults with rheumatoid arthritis.BioDrugs. 2014 Feb;28(1):75-106. doi: 10.1007/s40259-013-0076-8. BioDrugs. 2014. PMID: 24255004 Review.
Cited by
-
IL-6 receptor antagonist as adjunctive therapy with clotting factor replacement to protect against bleeding-induced arthropathy in hemophilia.J Thromb Haemost. 2013 May;11(5):881-93. doi: 10.1111/jth.12176. J Thromb Haemost. 2013. PMID: 23413986 Free PMC article.
-
The effect of disease-modifying antirheumatic drugs (DMARDs) on bone homeostasis in rheumatoid arthritis (RA) patients.Inflammopharmacology. 2023 Apr;31(2):689-697. doi: 10.1007/s10787-022-01088-7. Epub 2022 Nov 8. Inflammopharmacology. 2023. PMID: 36348208 Review.
-
Impact of senescence-associated secretory phenotype and its potential as a therapeutic target for senescence-associated diseases.Cancer Sci. 2017 Apr;108(4):563-569. doi: 10.1111/cas.13184. Epub 2017 Apr 18. Cancer Sci. 2017. PMID: 28165648 Free PMC article. Review.
-
Advances in rheumatology: new targeted therapeutics.Arthritis Res Ther. 2011 May 25;13 Suppl 1(Suppl 1):S5. doi: 10.1186/1478-6354-13-S1-S5. Arthritis Res Ther. 2011. PMID: 21624184 Free PMC article. Review.
-
Tocilizumab potentially prevents bone loss in patients with anticitrullinated protein antibody-positive rheumatoid arthritis.PLoS One. 2017 Nov 20;12(11):e0188454. doi: 10.1371/journal.pone.0188454. eCollection 2017. PLoS One. 2017. PMID: 29155868 Free PMC article.
References
-
- Lipsky PE, Heijde DM, St Clair EW, Furst DE, Breedveld FC, Kalden JR, et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. Anti-Tumor Necrosis Factor Trial in Rheumatoid Arthritis with Concomitant Therapy Study Group. N Engl J Med. 2000;343(22):1594–1602. doi: 10.1056/NEJM200011303432202. - DOI - PubMed
-
- Klareskog L, Heijde D, Jager JP, Gough A, Kalden J, Malaise M, et al. Therapeutic effect of the combination of etanercept and methotrexate compared with each treatment alone in patients with rheumatoid arthritis: double-blind randomised controlled trial. Lancet. 2004;363(9410):675–681. doi: 10.1016/S0140-6736(04)15640-7. - DOI - PubMed
-
- Keystone EC, Kavanaugh AF, Sharp JT, Tannenbaum H, Hua Y, Teoh LS, et al. Radiographic, clinical, and functional outcomes of treatment with adalimumab (a human anti-tumor necrosis factor monoclonal antibody) in patients with active rheumatoid arthritis receiving concomitant methotrexate therapy: a randomized, placebo-controlled, 52-week trial. Arthritis Rheum. 2004;50(5):1400–1411. doi: 10.1002/art.20217. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
