

Imaging three-dimensional myocardial mechanics using navigator-gated volumetric spiral cine DENSE MRI
- PMID: 20574967
- PMCID: PMC2946451
- DOI: 10.1002/mrm.22503
Imaging three-dimensional myocardial mechanics using navigator-gated volumetric spiral cine DENSE MRI
Abstract
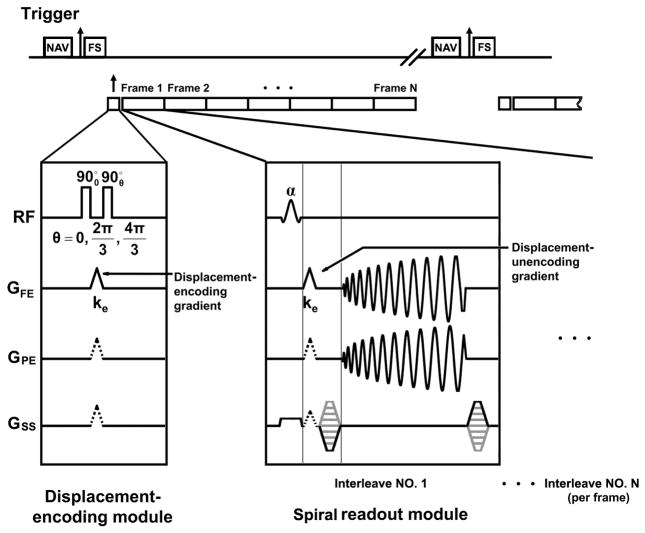
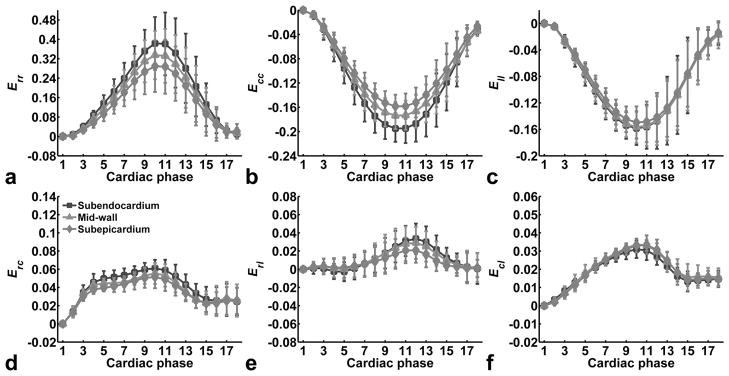
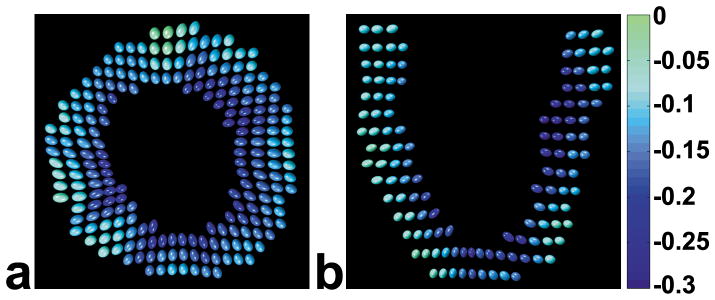
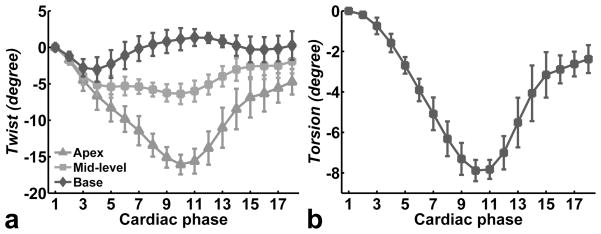
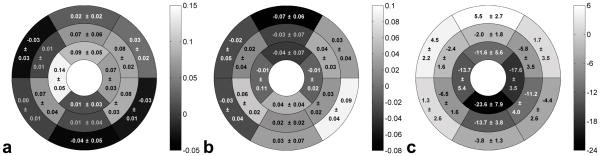
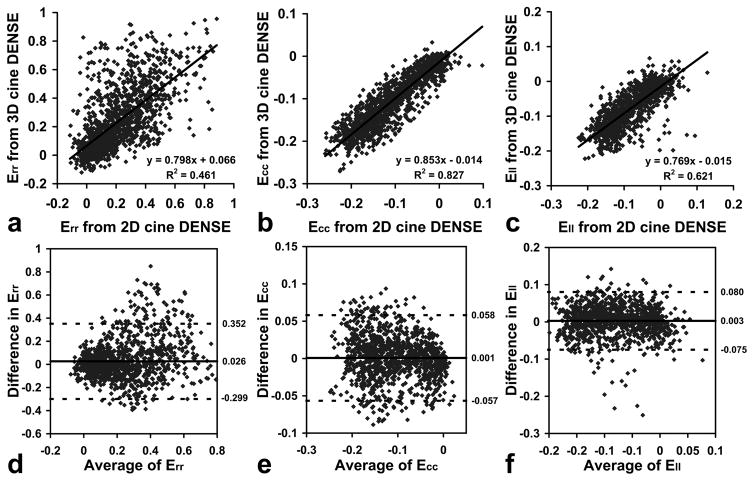
A navigator-gated 3D spiral cine displacement encoding with stimulated echoes (DENSE) pulse sequence for imaging 3D myocardial mechanics was developed. In addition, previously described 2D postprocessing algorithms including phase unwrapping, tissue tracking, and strain tensor calculation for the left ventricle (LV) were extended to 3D. These 3D methods were evaluated in five healthy volunteers, using 2D cine DENSE and historical 3D myocardial tagging as reference standards. With an average scan time of 20.5 ± 5.7 min, 3D data sets with a matrix size of 128 × 128 × 22, voxel size of 2.8 × 2.8 × 5.0 mm(3), and temporal resolution of 32 msec were obtained with displacement encoding in three orthogonal directions. Mean values for end-systolic mid-ventricular mid-wall radial, circumferential, and longitudinal strain were 0.33 ± 0.10, -0.17 ± 0.02, and -0.16 ± 0.02, respectively. Transmural strain gradients were detected in the radial and circumferential directions, reflecting high spatial resolution. Good agreement by linear correlation and Bland-Altman analysis was achieved when comparing normal strains measured by 2D and 3D cine DENSE. Also, the 3D strains, twist, and torsion results obtained by 3D cine DENSE were in good agreement with historical values measured by 3D myocardial tagging.
Figures
Similar articles
-
Optimal configuration of respiratory navigator gating for the quantification of left ventricular strain using spiral cine displacement encoding with stimulated echoes (DENSE) MRI.J Magn Reson Imaging. 2017 Mar;45(3):786-794. doi: 10.1002/jmri.25389. Epub 2016 Jul 26. J Magn Reson Imaging. 2017. PMID: 27458823 Free PMC article.
-
Myocardial 3D strain calculation by combining cine displacement encoding with stimulated echoes (DENSE) and cine strain encoding (SENC) imaging.Magn Reson Med. 2009 Jul;62(1):77-84. doi: 10.1002/mrm.21984. Magn Reson Med. 2009. PMID: 19322795 Free PMC article.
-
3D myocardial tissue tracking with slice followed cine DENSE MRI.J Magn Reson Imaging. 2008 May;27(5):1019-27. doi: 10.1002/jmri.21317. J Magn Reson Imaging. 2008. PMID: 18425823
-
Automated motion estimation for 2-D cine DENSE MRI.IEEE Trans Med Imaging. 2012 Sep;31(9):1669-81. doi: 10.1109/TMI.2012.2195194. Epub 2012 May 3. IEEE Trans Med Imaging. 2012. PMID: 22575669 Free PMC article. Review.
-
Myocardial tagging by cardiovascular magnetic resonance: evolution of techniques--pulse sequences, analysis algorithms, and applications.J Cardiovasc Magn Reson. 2011 Jul 28;13(1):36. doi: 10.1186/1532-429X-13-36. J Cardiovasc Magn Reson. 2011. PMID: 21798021 Free PMC article. Review.
Cited by
-
Society for Cardiovascular Magnetic Resonance 2019 Case of the Week series.J Cardiovasc Magn Reson. 2021 Apr 1;23(1):44. doi: 10.1186/s12968-020-00671-7. J Cardiovasc Magn Reson. 2021. PMID: 33794918 Free PMC article. Review.
-
Machine learning for multidimensional response and survival after cardiac resynchronization therapy using features from cardiac magnetic resonance.Heart Rhythm O2. 2022 Jun 17;3(5):542-552. doi: 10.1016/j.hroo.2022.06.005. eCollection 2022 Oct. Heart Rhythm O2. 2022. PMID: 36340495 Free PMC article.
-
Validation of cardiac magnetic-resonance-derived left ventricular strain measurements from free-breathing motion-corrected cine imaging.Pediatr Radiol. 2019 Jan;49(1):68-75. doi: 10.1007/s00247-018-4251-4. Epub 2018 Sep 22. Pediatr Radiol. 2019. PMID: 30244412 Free PMC article.
-
Comparison between conventional and compressed sensing cine cardiovascular magnetic resonance for feature tracking global circumferential strain assessment.J Cardiovasc Magn Reson. 2021 Feb 22;23(1):10. doi: 10.1186/s12968-021-00708-5. J Cardiovasc Magn Reson. 2021. PMID: 33618722 Free PMC article.
-
Imaging of early modification in cardiomyopathy: the doxorubicin-induced model.Int J Cardiovasc Imaging. 2013 Oct;29(7):1459-76. doi: 10.1007/s10554-013-0248-0. Epub 2013 Jun 7. Int J Cardiovasc Imaging. 2013. PMID: 23744127 Review.
References
-
- Korosoglou G, Futterer S, Humpert PM, Riedle N, Lossnitzer D, Hoerig B, Steen H, Giannitsis E, Osman NF, Katus HA, Korosoglou G, Futterer S, Humpert PM, Riedle N, Lossnitzer D, Hoerig B, Steen H, Giannitsis E, Osman NF, Katus HA. Strain-encoded cardiac MR during high-dose dobutamine stress testing: comparison to cine imaging and to myocardial tagging. J Magn Reson Imaging. 2009;29(5):1053–1061. - PubMed
-
- Bansal M, Cho GY, Chan J, Leano R, Haluska BA, Marwick TH. Feasibility and accuracy of different techniques of two-dimensional speckle based strain and validation with harmonic phase magnetic resonance imaging. J Am Soc Echocardiogr. 2008;21(12):1318–1325. - PubMed
-
- Setser RM, Smedira NG, Lieber ML, Sabo ED, White RD. Left ventricular torsional mechanics after left ventricular reconstruction surgery for ischemic cardiomyopathy. J Thorac Cardiovasc Surg. 2007;134(4):888–896. - PubMed
-
- Setser RM, White RD, Sturm B, McCarthy PM, Starling RC, Young JB, Kasper J, Buda T, Obuchowski N, Lieber ML. Noninvasive assessment of cardiac mechanics and clinical outcome after partial left ventriculectomy. Ann Thorac Surg. 2003;76(5):1576–1585. - PubMed
-
- Kramer CM, Magovern JA, Rogers WJ, Vido D, Savage EB. Reverse remodeling and improved regional function after left ventricular aneurysm repair. J Thorac Cardiovasc Surg. 2002;123(4):700–706. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
