

The psychophysiology of blood-injection-injury phobia: looking beyond the diphasic response paradigm
- PMID: 20576505
- PMCID: PMC6688615
- DOI: 10.1016/j.ijpsycho.2010.05.007
The psychophysiology of blood-injection-injury phobia: looking beyond the diphasic response paradigm
Abstract
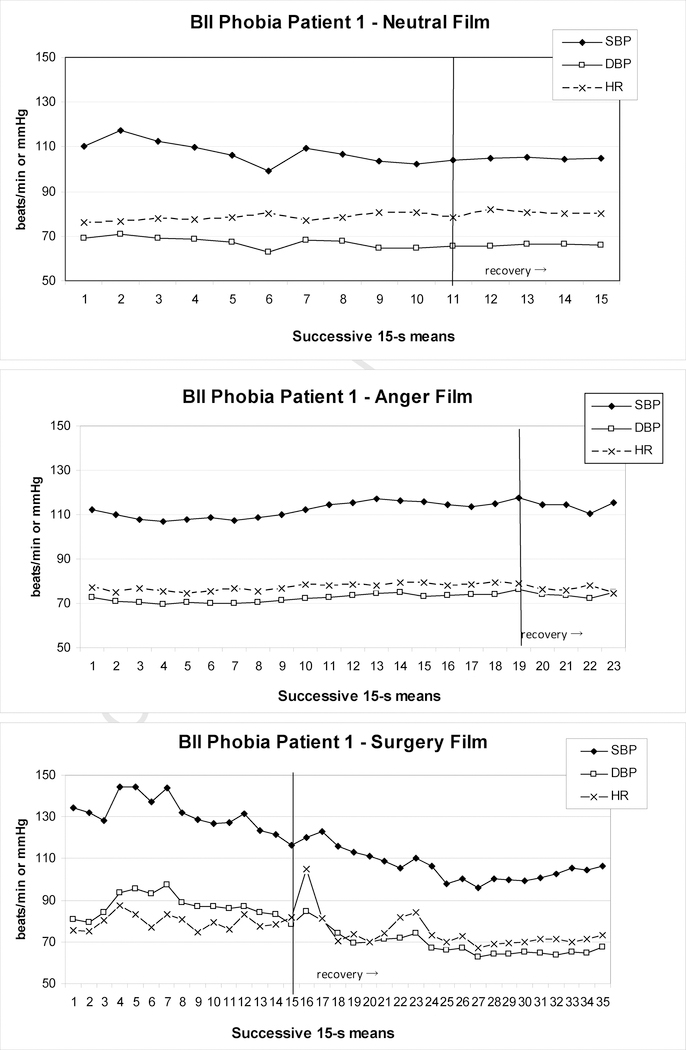
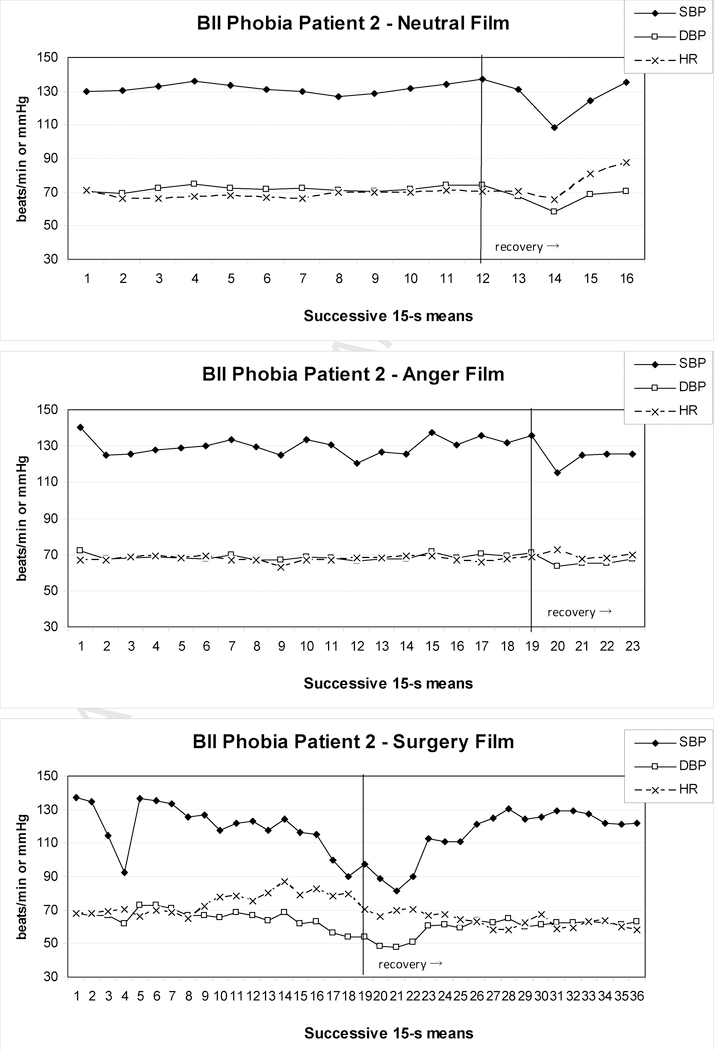
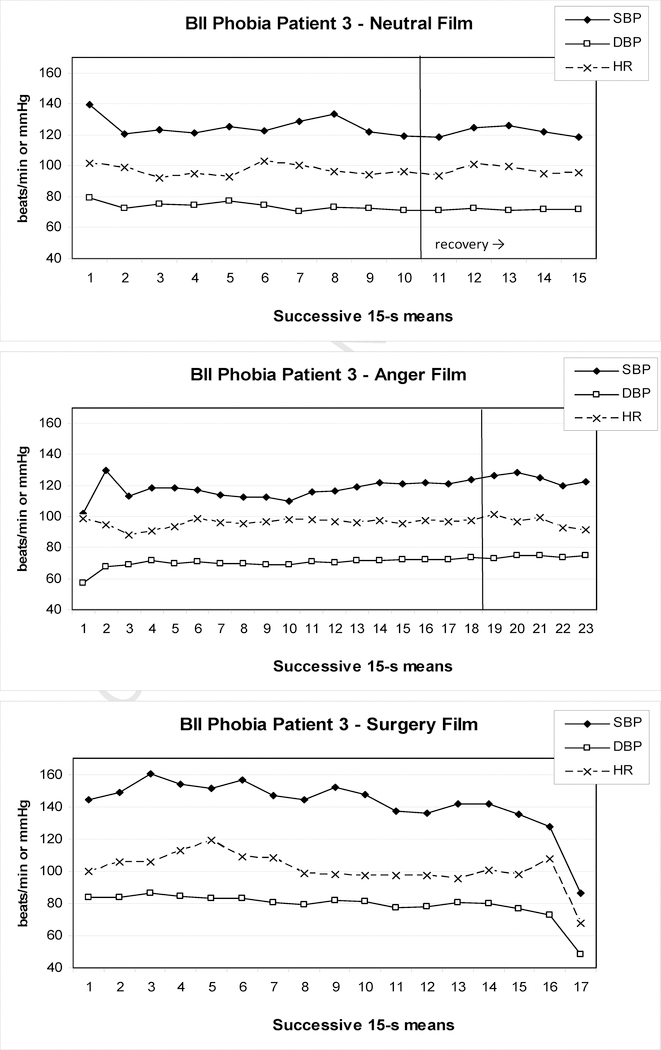
Blood-injection-injury (BII) phobia is an anxiety disorder that may be accompanied by vasovagal fainting during confrontation with the feared stimuli. The underlying pattern of autonomic regulation has been characterized as a diphasic response, with initial increases in heart rate and blood pressure that are typical of a fight-flight response, and subsequent drops in blood pressure and/or heart rate that may precipitate vasovagal fainting. Tensing skeletal muscles of the arms, legs, and trunk (applied tension) has been proposed as a technique to cope with this dysregulation. This review critically examines the empirical basis for the diphasic response and its treatment by applied tension in BII phobia. An alternative perspective on the psychophysiology of BII phobia and vasovagal fainting is offered by focusing on hypocapnia that leads to cerebral blood flow reductions, a perspective supported by research on neurocardiogenic and orthostatically-induced syncope. The evidence may indicate a role for respiration-focused coping techniques in BII phobia.
2010 Elsevier B.V. All rights reserved.
Figures
Similar articles
-
[Blood-injection-injury phobia: Physochophysiological and therapeutical specificities].Encephale. 2013 Oct;39(5):326-31. doi: 10.1016/j.encep.2012.06.031. Epub 2012 Sep 25. Encephale. 2013. PMID: 23095595 French.
-
Cardiovascular activity in blood-injection-injury phobia during exposure: evidence for diphasic response patterns?Behav Res Ther. 2013 Aug;51(8):460-8. doi: 10.1016/j.brat.2013.03.011. Epub 2013 Apr 23. Behav Res Ther. 2013. PMID: 23747585
-
Diminished medial prefrontal cortex activity in blood-injection-injury phobia.Biol Psychol. 2007 May;75(2):124-30. doi: 10.1016/j.biopsycho.2007.01.002. Epub 2007 Jan 19. Biol Psychol. 2007. PMID: 17306437
-
Predisposition to vasovagal syncope in subjects with blood/injury phobia.Circulation. 2001 Aug 21;104(8):903-7. doi: 10.1161/hc3301.094910. Circulation. 2001. PMID: 11514377 Clinical Trial.
-
Treatments for blood-injury-injection phobia: a critical review of current evidence.J Psychiatr Res. 2009 Oct;43(15):1235-42. doi: 10.1016/j.jpsychires.2009.04.008. Epub 2009 May 22. J Psychiatr Res. 2009. PMID: 19464700 Review.
Cited by
-
Hyperventilation in panic disorder and asthma: empirical evidence and clinical strategies.Int J Psychophysiol. 2010 Oct;78(1):68-79. doi: 10.1016/j.ijpsycho.2010.05.006. Epub 2010 May 25. Int J Psychophysiol. 2010. PMID: 20685222 Free PMC article. Review.
-
Phlebotomy, a bridge between laboratory and patient.Biochem Med (Zagreb). 2016;26(1):17-33. doi: 10.11613/BM.2016.002. Biochem Med (Zagreb). 2016. PMID: 26981016 Free PMC article. Review.
-
Late cortical positivity and cardiac responsitivity in female dental phobics when exposed to phobia-relevant pictures.Int J Psychophysiol. 2011 Mar;79(3):410-6. doi: 10.1016/j.ijpsycho.2011.01.003. Epub 2011 Jan 14. Int J Psychophysiol. 2011. PMID: 21238507 Free PMC article.
-
Interventions for Individuals With High Levels of Needle Fear: Systematic Review of Randomized Controlled Trials and Quasi-Randomized Controlled Trials.Clin J Pain. 2015 Oct;31(10 Suppl):S109-23. doi: 10.1097/AJP.0000000000000273. Clin J Pain. 2015. PMID: 26352916 Free PMC article.
-
The clinical characterization of the adult patient with an anxiety or related disorder aimed at personalization of management.World Psychiatry. 2021 Oct;20(3):336-356. doi: 10.1002/wps.20919. World Psychiatry. 2021. PMID: 34505377 Free PMC article.
References
-
- Abelson JL, Weg JG, Nesse RM, Curtis GC, 2001. Persistent respiratory irregularity in patients with panic disorder. Biological Psychiatry 49, 588–595. - PubMed
-
- Abu-Shaweesh JM, Martin RJ, 2008. Neonatal apnea: what’s new? Pediatric Pulmonology 43, 937–44. - PubMed
-
- Accurso V, Winnicki M, Shamsuzzaman AS, Wenzel A, Johnson AK, Somers VK, 2001. Predisposition to vasovagal syncope in subjects with blood/injury phobia. Circulation 104, 903–907. - PubMed
-
- Ader PSJ, France C, Ditto B, 1991. Baroreflex sensitivity at rest and during stress in individuals with a history of vasovagal syncope. Journal of Psychosomatic Research 35, 591–597. - PubMed
-
- Alboni P, Alboni M, Bertorelle G, 2008. The origin of vasovagal syncope: to protect the heart or to escape predation? Clinical Autonomic Research 18, 170–178. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
