

Increased mortality in hypernatremic burned patients
- PMID: 20577644
- PMCID: PMC2890210
- DOI: 10.3205/000100
Increased mortality in hypernatremic burned patients
Abstract
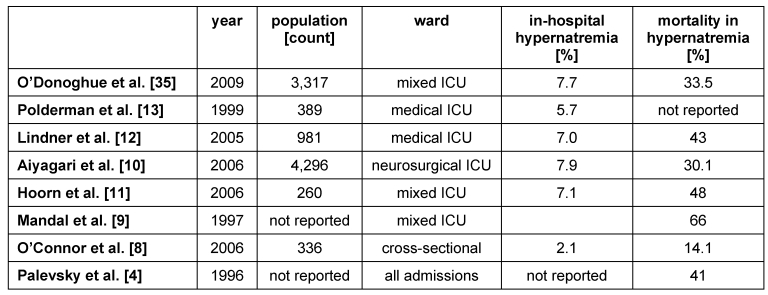
Introduction: In-hospital hypernatremia develops usually iatrogenically from inadequate or inappropriate fluid prescription. In severely burned patient an extensive initial fluid resuscitation is necessary for burn shock survival. After recovering of cellular integrity the circulating volume has to be normalized. Hereby extensive water and electrolyte shifts can provoke hypernatremia.
Purpose: Is a hypernatremic state associated with increased mortality?
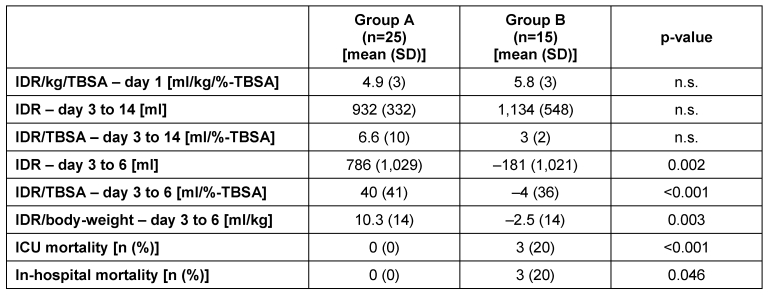
Method: Retrospective study for the incidence of hypernatremia and survival in 40 patients with a totally burned surface area (TBSA) >10%. Age, sex, TBSA, ABSI-Score and fluid resuscitation within the first 24 hours were analyzed. Patients were separated in two groups without (Group A) or with (Group B) hypernatremia.
Results: Hypernatremia occurred on day 5+/-1.4. No significant difference for age, sex, TBSA, ABSI-Score and fluid resuscitation within the first 24 hours were calculated. In Group A all patients survived, while 3 of the hypernatremic patient in Group B died during ICU-stay (Odds-ratio = 1.25; 95% CI 0.971-1.61; p=0.046).
Conclusion: Burned patients with an in-hospital acquired hypernatremia have an increased mortality risk. In case of a hypernatremic state early intervention is obligatory. There is a need of a fluid removal strategy in severely burned patient to avoid water imbalance.
Einführung: Im Krankenhaus auftretende Hypernatriämien werden häufig iatrogen durch unzureichende Flüssigkeitstherapie hervorgerufen. Schwerbrandverletzte Patienten benötigen große Mengen an Flüssigkeitssubstitution während des Verbrennungsschocks. Nach Verschluss des Kapillarlecks muss das zirkulierende Volumen wieder normalisiert werden. Durch die Verschiebung großer Mengen an Flüssigkeit und Elektrolyten können Hypernatriämien provoziert werden.
Fragestellung: Haben Schwerbrandverletzte mit einer Hypernatriämie eine erhöhte Mortalitätsrate?
Methoden: Retrospektive Studie an 40 Schwerbrandverletzten (verbrannte Körperoberfläche (TBSA) >10%). Alter, Geschlecht, TBSA, ABSI, Mortalität und Flüssigkeitssubstitution (während der ersten 24 Stunden) wurden auf eine Assoziation mit einer Hypernatriämie untersucht. Es erfolgte die Differenzierung in Gruppe A (keine Hypernatriämie) und Gruppe B (Hypernatriämie).
Ergebnisse: Eine Hypernatriämie wurde im Mittel am 5. (±1,4) Tag festgestellt. Es zeigten sich keine signifikanten Unterschiede bzgl. Alter, Geschlecht, TBSA, ABSI und Flüssigkeitsbedarf (in den ersten 24 Stunden). Alle Patienten in Gruppe A überlebten. In Gruppe B starben 3 Patienten (Odds-ratio = 1,25; 95% Konfidenzintervall 0,971–1,61; p=0,046).
Schlussfolgerung: Schwerbrandverletzte mit einer Hypernatriämie haben eine erhöhte Mortalität. Neben der engmaschigen Kontrolle ist eine frühe Therapie von Hypernatriämien obligat.
Keywords: burn injury; critical care; hypernatremia; mortality.
Figures


References
-
- Gennari FJ. Current concepts: Serum osmolality: Uses and limitations. N Engl J Med. 1984;310(2):102–105. - PubMed
-
- Adrogue HJ, Madias NE. Hypernatremia. N Engl J Med. 2000;342(20):1493–1499. doi: 10.1056/NEJM200005183422006. Available from: http://dx.doi.org/10.1056/NEJM200005183422006. - DOI - PubMed
-
- Snyder NA, Feigal DW, Arieff AI. Hypernatremia in elderly patients: A heterogeneous, morbid, and iatrogenic entity. Ann Intern Med. 1987;107(3):309–319. - PubMed
-
- Palevsky PM, Bhagrath R, Greenberg A. Hypernatremia in hospitalized patients. Ann Intern Med. 1996;124(2):197–203. - PubMed
-
- Lin M, Liu SJ, Lim IT. Disorders of water imbalance. Emerg Med Clin North Am. 2005;23(3):749–70, ix. doi: 10.1016/j.emc.2005.03.001. Available from: http://dx.doi.org/10.1016/j.emc.2005.03.001. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
