

Early postoperative alterations of ventilation parameters after tracheostomy in major burn injuries
- PMID: 20577645
- PMCID: PMC2890211
- DOI: 10.3205/000099
Early postoperative alterations of ventilation parameters after tracheostomy in major burn injuries
Abstract
Purpose: In patients with major burn injuries mechanical ventilation is often required for longer periods. Tracheostomy (TS) plays an integral role in airway management. We investigated the effect of TS on ventilation parameters within 8 hours after TS.
Materials: A retrospective analysis of severely burned patients admitted to the burn unit of a German University Hospital was performed. Ventilation parameters 8 hours before and after TS were registered.
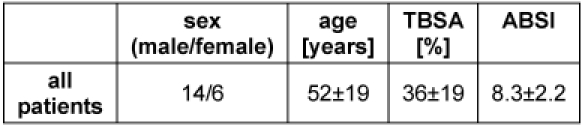
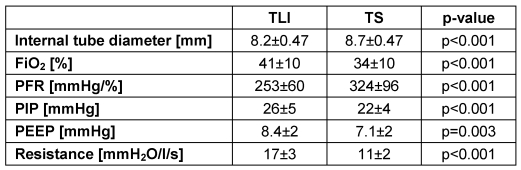
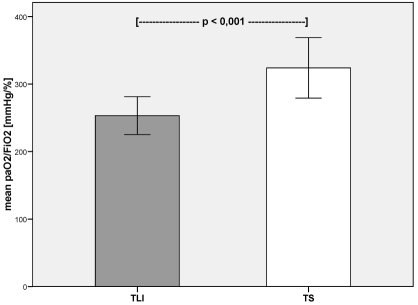
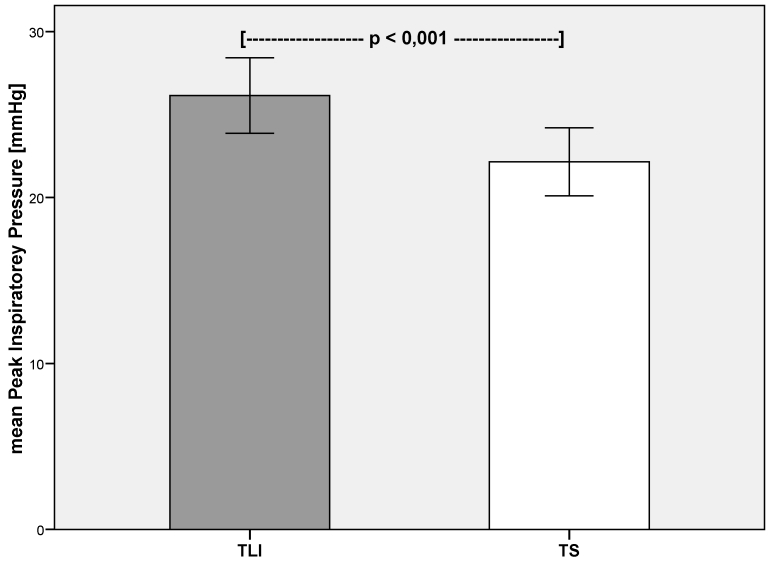
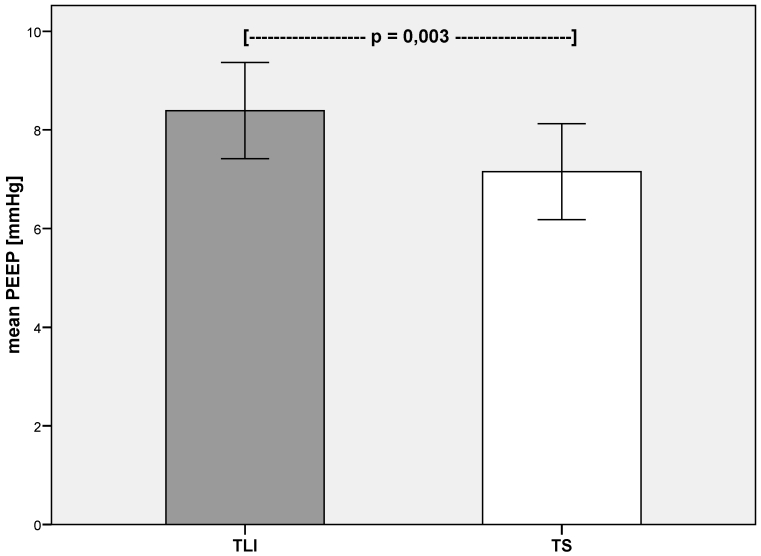
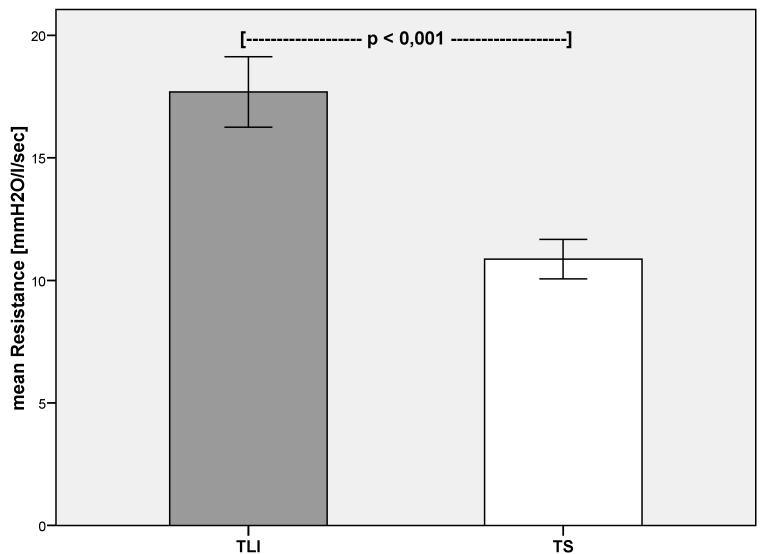
Results: A retrospective analysis of 20 patients which received surgical TS was performed. Mean age was 52+/-19 years. Mean abbreviated burned severity index (ABSI) was 8.3+/-2.2. A mechanical ventilation was required for 14.3+/-4.8 days. TS was performed on day 7+/-4. Inspiratory oxygen concentration (FiO(2)) (p<0.001), peak inspiratory pressure (p<0.001), positive end-expiratory pressure (p=0.003) and pulmonary resistance (p<0.001) were reduced significantly after TS. The arterial partial pressure of oxygen/FiO(2)-ratio increased significantly after TS (p<0.001).
Conclusions: We demonstrate that TS reduces invasiveness of ventilation in severely burned patients and by this can optimize lung protective ventilation strategy.
Einleitung: Schwerbrandverletzte müssen häufig langfristig maschinell beatmet werden. Die Tracheostomie (TS) hat einen hohen Stellenwert in der Langzeitbeatmung. Wir untersuchen, ob eine Veränderung der Beatmungsparameter innerhalb von 8 Stunden nach TS festzustellen ist.
Material und Methoden: Retrospektive Analyse an schwerbrandverletzten Patienten einer deutschen Intensiveinheit für Schwerbrandverletzte. Die Beatmungsparameter wurden 8 Stunden vor und 8 Stunden nach der TS ausgewertet.
Ergebnisse: 20 Patienten mit einem mittleren Alter von 52±19 Jahren wurden eingeschlossen. Der mittlere ABSI-Wert betrug 8,3±2,2. Die mittlere Beatmungsdauer betrug 14,3±4,8 Tage. Die TS wurde im Mittel am 7. (±4) posttraumatischen Tag durchgeführt. Die inspiratorische Sauerstoffkonzentration (FiO2) (p<0,001), der inspiratorische Spitzendruck (p<0,001), der positive end-exspiratorische Druck (p=0,003) und der pulmonale Widerstand (p<0,001) waren innerhalb von 8 Stunden nach TS signifikant reduziert. Das Verhältnis von arteriellem Sauerstoffpartialdruck und FiO2 stieg innerhalb von 8 Stunden postoperativ signifikant an (p<0,001).
Schlussfolgerung: Wir konnten zeigen, dass frühzeitig nach einer TS eine reduzierte Invasivität der maschinellen Beatmung erreicht wird und somit die lungenprotektive Beatmungsstrategie optimiert werden kann.
Keywords: critical care; intensive care; pulmonary gas exchange; pulmonary ventilation; tracheostomy.
Figures
References
-
- Ross BJ, Barker DE, Russell WL, Burns RP. Prediction of long-term ventilatory support in trauma patients. Am Surg. 1996;62(1):19–25. - PubMed
-
- Bert JL, Bowen BD, Reed RK, Onarheim H. Microvascular exchange during burn injury: IV; Fluid resuscitation model. Circ Shock. 1991;34(3):285–297. - PubMed
-
- Lund T, Bert JL, Onarheim H, Bowen BD, Reed RK. Microvascular exchange during burn injury; I: A review. Circ Shock. 1989;28(3):179–197. - PubMed
-
- Soejima K, Schmalstieg FC, Sakurai H, Traber LD, Traber DL. Pathophysiological analysis of combined burn and smoke inhalation injuries in sheep. Am J Physiol Lung Cell Mol Physiol. 2001;280(6):L1233–L1241. - PubMed
-
- Enkhbaatar P, Traber DL. Pathophysiology of acute lung injury in combined burn and smoke inhalation injury. Clin Sci (Lond) 2004;107(2):137–143. doi: 10.1042/CS20040135. Available from: http://dx.doi.org/10.1042/CS20040135. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
