

Clinical implications of microvascular obstruction and intramyocardial haemorrhage in acute myocardial infarction using cardiovascular magnetic resonance imaging
- PMID: 20577881
- PMCID: PMC2948162
- DOI: 10.1007/s00330-010-1849-9
Clinical implications of microvascular obstruction and intramyocardial haemorrhage in acute myocardial infarction using cardiovascular magnetic resonance imaging
Abstract
Objectives: To investigate the clinical implications of microvascular obstruction (MVO) and intramyocardial haemorrhage (IMH) in acute myocardial infarction (AMI).
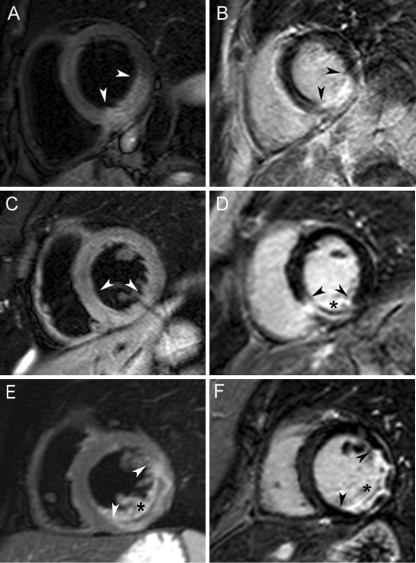
Methods: Ninety patients with a first AMI undergoing primary percutaneous coronary intervention (PCI) were studied. T2-weighted, cine and late gadolinium-enhanced cardiovascular magnetic resonance imaging was performed at 5 ± 2 and 103 ± 11 days. Patients were categorised into three groups based on the presence or absence of MVO and IMH.
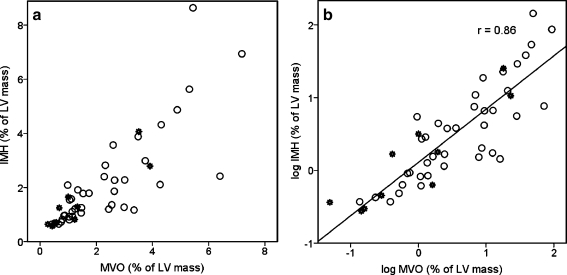
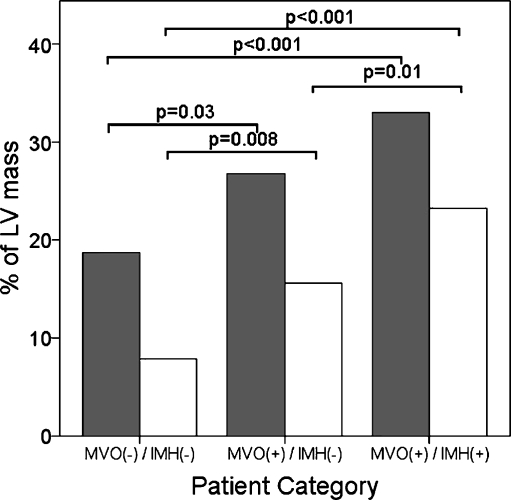
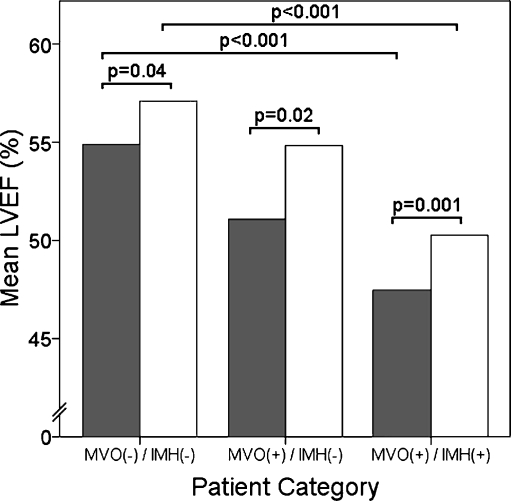
Results: MVO was observed in 54% and IMH in 43% of patients, and correlated significantly (r = 0.8, p < 0.001). Pre-PCI thrombolysis in myocardial infarction 3 flow was only observed in MVO(-)/IMH(-) patients. Infarct size and impairment of systolic function were largest in MVO(+)/IMH(+) patients (n = 39, 23 ± 9% and 47 ± 7%), smallest in MVO(-)/IMH(-) patients (n = 41, 8 ± 8% and 55 ± 8%) and intermediate in MVO(+)/IMH(-) patients (n = 10, 16 ± 7% and 51 ± 6%, p < 0.001). LVEF increased in all three subgroups at follow-up, but remained intermediate in MVO(+)/IMH(-) and was lowest in MVO(+)/IMH(+) patients. Using random intercept model analysis, only infarct size was an independent predictor for adverse LV remodelling.
Conclusions: Intramyocardial haemorrhage and microvascular obstruction are strongly related. Pre-PCI TIMI 3 flow is less frequently observed in patients with MVO and IMH. Only infarct size was an independent predictor of LV remodelling.
Figures
References
-
- Reimer KA, Lowe JE, Rasmussen MM, et al. The wavefront phenomenon of ischemic cell death. 1. Myocardial infarct size vs duration of coronary occlusion in dogs. Circulation. 1977;56:786–794. - PubMed
-
- Fishbein MC, J Y-Rit, Lando U, et al. The relationship of vascular injury and myocardial hemorrhage to necrosis after reperfusion. Circulation. 1980;62:1274–1279. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
