

Anxiety as a predictor of treatment outcome in children and adolescents with depression
- PMID: 20578934
- PMCID: PMC2936256
- DOI: 10.1089/cap.2010.0006
Anxiety as a predictor of treatment outcome in children and adolescents with depression
Abstract
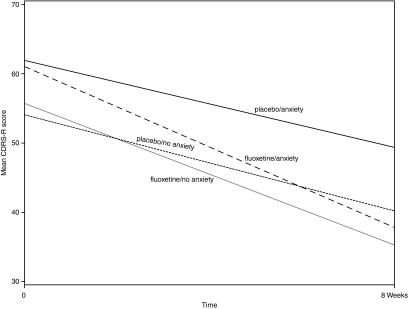
Objective: The aim of this study was to examine the impact of co-morbid illnesses on treatment outcomes in depressed children and adolescents aged 7-17 who were treated with fluoxetine.
Method: This data set was drawn from two large clinical trials involving children and adolescents with depression. Subjects with a diagnosis of major depressive disorder and depressive symptoms of at least moderate severity as defined by a Children's Depression Rating Score, Revised (CDRS-R) total score >or=40 and a Clinical Global Impressions-Severity (CGI-S) rating >or=4 were included. Subjects were randomized to receive fluoxetine or placebo over an 8-week period. Predictor analyses examining two primary outcomes were conducted: (1) Response based on Clinical Global Impressions-Improvement (CGI-I) score of 1 or 2, and (2) remission based on CDRS-R score of <or=28. Logistic regression models were run to assess whether anxiety disorders were a predictor of response or remission.
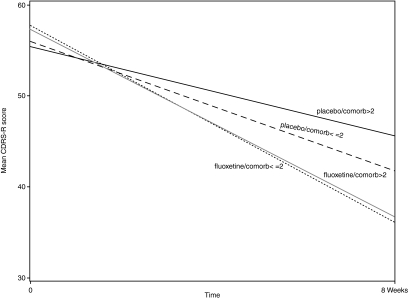
Result: A total of 309 study participants were included. The only factor found to influence response was treatment with fluoxetine (p = 0.022, odds ratio [OR] = 2.08, 95% confidence interval [CI] 1.30, 3.31). Several factors were found to influence remission: Treatment with fluoxetine (p < 0.0001, OR = 3.17, 95% CI 1.80, 5.57), gender (p = 0.024, OR = 1.90, 95% CI 1.09, 3.30), and number of co-morbid diagnoses (p = 0.026, OR 0.73, 95% CI 0.55, 0.96).
Conclusion: Anxiety disorders alone did not predict response or remission, but the total number of co-morbid illnesses was associated with remission in depressed children and adolescents treated with fluoxetine.
Figures
Similar articles
-
Desvenlafaxine Versus Placebo in a Fluoxetine-Referenced Study of Children and Adolescents with Major Depressive Disorder.J Child Adolesc Psychopharmacol. 2018 Feb;28(1):36-46. doi: 10.1089/cap.2017.0100. Epub 2017 Nov 30. J Child Adolesc Psychopharmacol. 2018. PMID: 29189044 Free PMC article. Clinical Trial.
-
Do children and adolescents have differential response rates in placebo-controlled trials of fluoxetine?CNS Spectr. 2007 Feb;12(2):147-54. doi: 10.1017/s1092852900020666. CNS Spectr. 2007. PMID: 17277715
-
Fluoxetine treatment of depressed patients with comorbid anxiety disorders.J Psychopharmacol. 2002 Sep;16(3):215-9. doi: 10.1177/026988110201600304. J Psychopharmacol. 2002. PMID: 12236627
-
Meta-analysis of aggression and/or hostility-related events in children and adolescents treated with fluoxetine compared with placebo.J Child Adolesc Psychopharmacol. 2007 Oct;17(5):713-8. doi: 10.1089/cap.2006.0138. J Child Adolesc Psychopharmacol. 2007. PMID: 17979590 Review.
-
Can Fluoxetine Combined with Cognitive Behavioral Therapy Reduce the Suicide and Non-Suicidal Self-Injury Incidence and Recurrence Rate in Depressed Adolescents Compared with Fluoxetine Alone? A Meta-Analysis.Neuropsychiatr Dis Treat. 2022 Nov 2;18:2543-2557. doi: 10.2147/NDT.S367931. eCollection 2022. Neuropsychiatr Dis Treat. 2022. PMID: 36349346 Free PMC article. Review.
Cited by
-
Cool Kids: Cognitive Behavioral Therapy in a Spanish Sample of Children and Adolescents with Anxiety Disorders.Child Psychiatry Hum Dev. 2025 Jun;56(3):751-757. doi: 10.1007/s10578-023-01579-w. Epub 2023 Sep 6. Child Psychiatry Hum Dev. 2025. PMID: 37672194
-
Identifying factors associated with the hospital readmission rate among patients with major depressive disorder.BMC Psychiatry. 2021 Nov 1;21(1):542. doi: 10.1186/s12888-021-03559-7. BMC Psychiatry. 2021. PMID: 34724910 Free PMC article.
-
Psychometric Properties of the Patient Health Questionnaire-9 Modified for Major Depressive Disorder in Adolescents.J Child Adolesc Psychopharmacol. 2019 Feb;29(1):34-40. doi: 10.1089/cap.2018.0112. Epub 2018 Nov 2. J Child Adolesc Psychopharmacol. 2019. PMID: 30388048 Free PMC article.
-
Factors associated with failure to achieve remission and with relapse after remission in patients with major depressive disorder in the PERFORM study.Neuropsychiatr Dis Treat. 2017 Aug 9;13:2151-2165. doi: 10.2147/NDT.S136343. eCollection 2017. Neuropsychiatr Dis Treat. 2017. PMID: 28860772 Free PMC article.
-
Substance use and internalizing symptoms among high school students and access to health care services: results from a population-based study.Can J Public Health. 2019 Feb;110(1):85-92. doi: 10.17269/s41997-018-0144-4. Epub 2018 Nov 7. Can J Public Health. 2019. PMID: 30406338 Free PMC article.
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed. Revised (DSM-III-R) Washington (DC): American Psychiatric Association; 1987.
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) Washington (DC): American Psychiatric Association; 1994.
-
- Angold A. Costello EJ. Erkanli A. Comorbidity. J Child Psychol Psychiatry. 1999;40:57–87. - PubMed
-
- Asarnow JR. Emslie G. Clarke G. Wagner KD. Spirito A. Vitiello B. Iyengar S. Shamseddeen W. Ritz L. Mccracken J. Strober M. Suddath R. Leonard H. Porta G. Keller M. Brent D. Treatment of selective serotonin reuptake inhibitor-resistant depression in adolescents: Predictors and moderators of treatment response. J Am Acad Child Adolesc Psychiatry. 2009;48:330–339. - PMC - PubMed
-
- Brent DA. Kolko DJ. Birmaher B. Baugher M. Brige J. Roth C. Holder D. Predictors of treatment efficacy in a clinical trial of three psychosocial treatments for adolescent depression. J Am Acad Child Adolesc Psychiatry. 1998;37:906–914. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
