

Dietary potassium intake and mortality in long-term hemodialysis patients
- PMID: 20580474
- PMCID: PMC2910783
- DOI: 10.1053/j.ajkd.2010.03.022
Dietary potassium intake and mortality in long-term hemodialysis patients
Abstract
Background: Hyperkalemia has been associated with higher mortality in long-term hemodialysis (HD) patients. There are few data concerning the relationship between dietary potassium intake and outcome.
Study design: The mortality predictability of dietary potassium intake from reported food items estimated using the Block Food Frequency Questionnaire (FFQ) at the start of the cohort was examined in a 5-year (2001-2006) cohort of 224 HD patients in Southern California using Cox proportional hazards regression.
Setting & participants: 224 long-term HD patients from 8 DaVita dialysis clinics.
Predictors: Dietary potassium intake ranking using the Block FFQ.
Outcomes: 5-year survival.
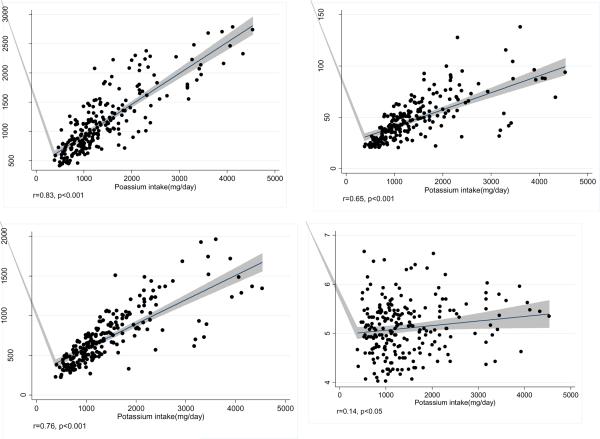
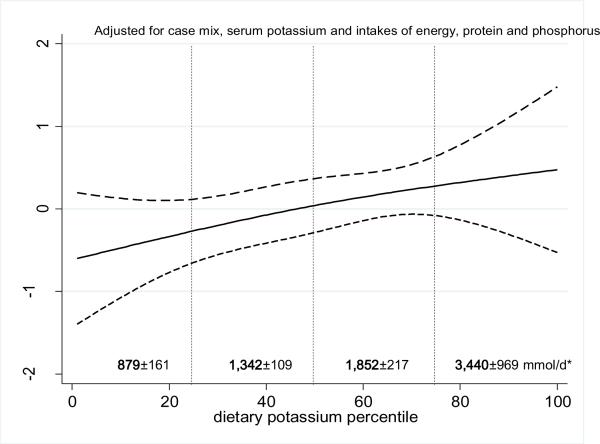
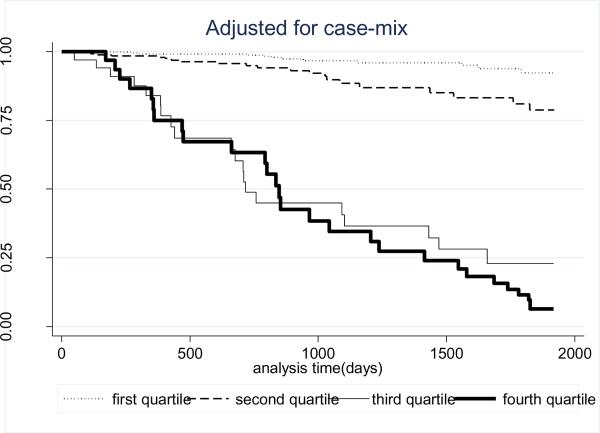
Results: HD patients with higher potassium intake had greater dietary energy, protein, and phosphorus intakes and higher predialysis serum potassium and phosphorus levels. Greater dietary potassium intake was associated with significantly increased death HRs in unadjusted models and after incremental adjustments for case-mix, nutritional factors (including 3-month averaged predialysis serum creatinine, potassium, and phosphorus levels; body mass index; normalized protein nitrogen appearance; and energy, protein, and phosphorus intake) and inflammatory marker levels. HRs for death across the 3 higher quartiles of dietary potassium intake in the fully adjusted model (compared with the lowest quartile) were 1.4 (95% CI, 0.6-3.0), 2.2 (95% CI, 0.9-5.4), and 2.4 (95% CI, 1.1-7.5), respectively (P for trend = 0.03). Restricted cubic spline analyses confirmed the incremental mortality predictability of higher potassium intake.
Limitations: FFQs may underestimate individual potassium intake and should be used to rank dietary intake across the population.
Conclusions: Higher dietary potassium intake is associated with increased death risk in long-term HD patients, even after adjustments for serum potassium level; dietary protein; energy, and phosphorus intake; and nutritional and inflammatory marker levels. The potential role of dietary potassium in the high mortality rate of HD patients warrants clinical trials.
Copyright (c) 2010 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Port FK. Morbidity and mortality in dialysis patients. Kidney Int. 1994;46:1728–37. - PubMed
-
- Iseki K, Kawazoe N, Osawa A, Fukiyama K. Survival analysis of dialysis patients in Okinawa, Japan (1971–1990) Kidney Int. 1993;43:404–9. - PubMed
-
- Berl T, Henrich W. Kidney-heart interactions: epidemiology, pathogenesis, and treatment. Clin J Am Soc Nephrol. 2006;1:8–18. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–305. - PubMed
-
- Lowrie EG, Lew NL. Death risk in hemodialysis patients: the predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am J Kidney Dis. 1990;15:458–82. - PubMed
