

Familial C4B deficiency and immune complex glomerulonephritis
- PMID: 20580617
- PMCID: PMC2941544
- DOI: 10.1016/j.clim.2010.06.003
Familial C4B deficiency and immune complex glomerulonephritis
Abstract
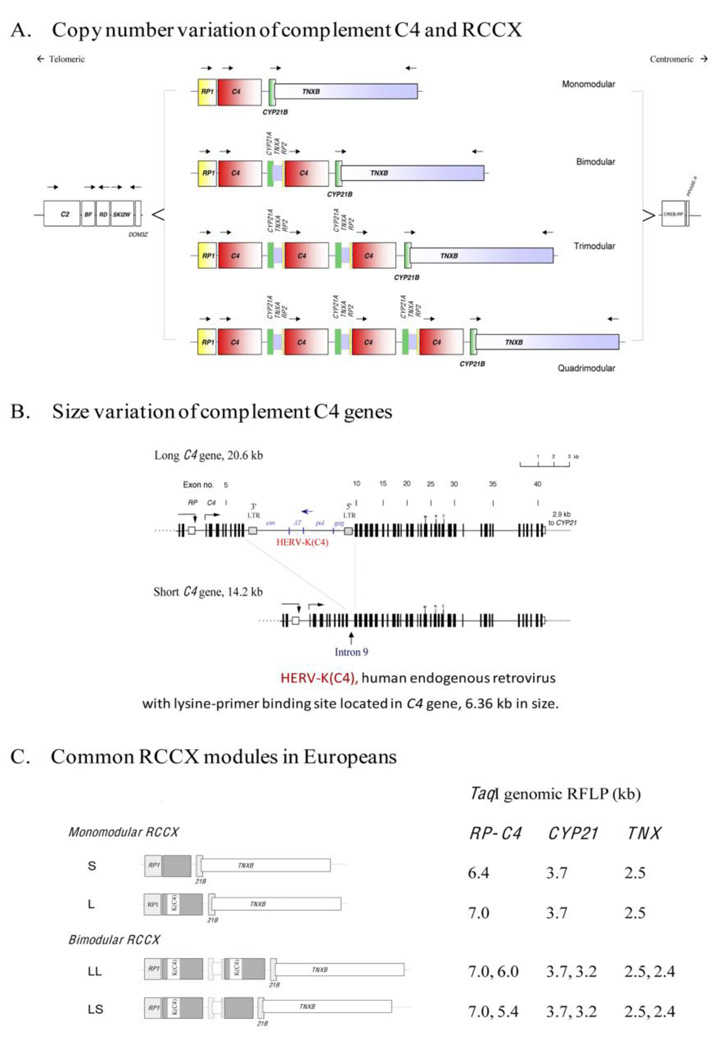
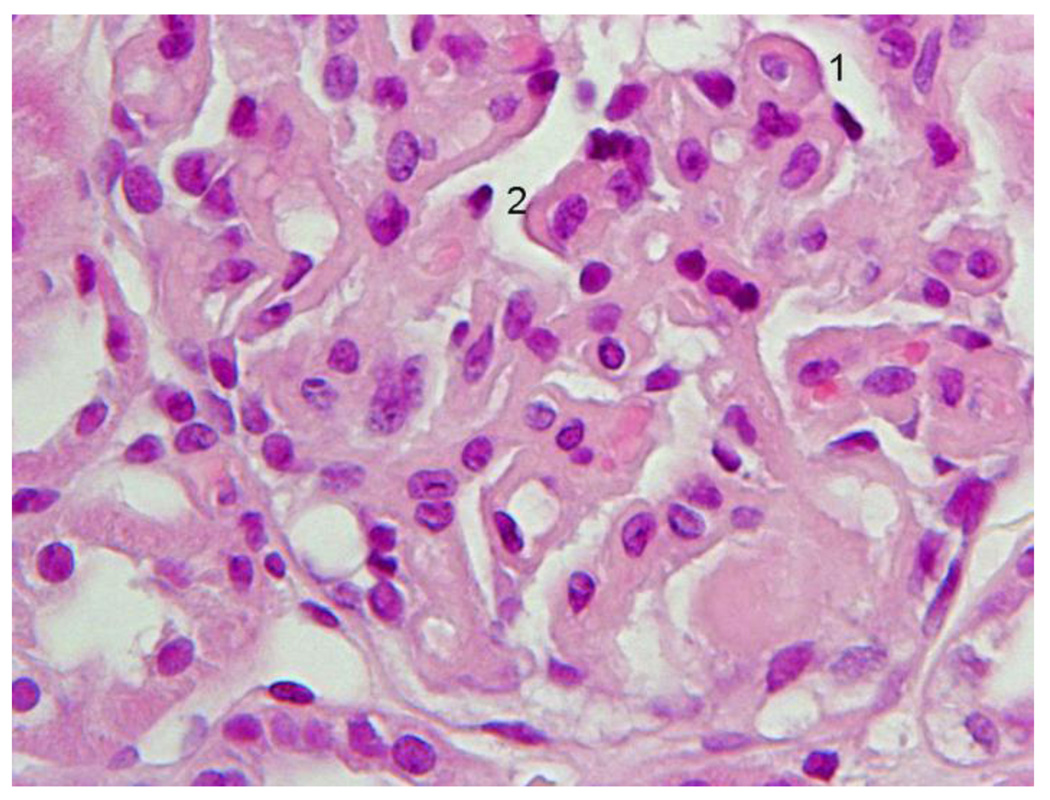
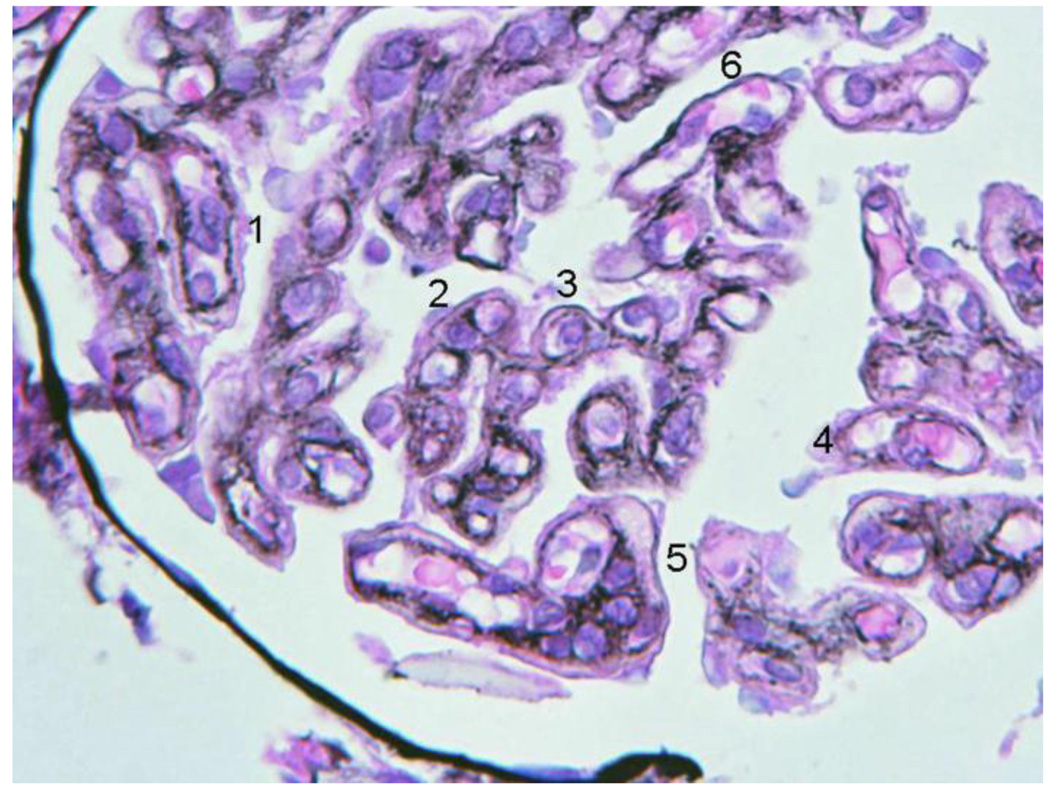
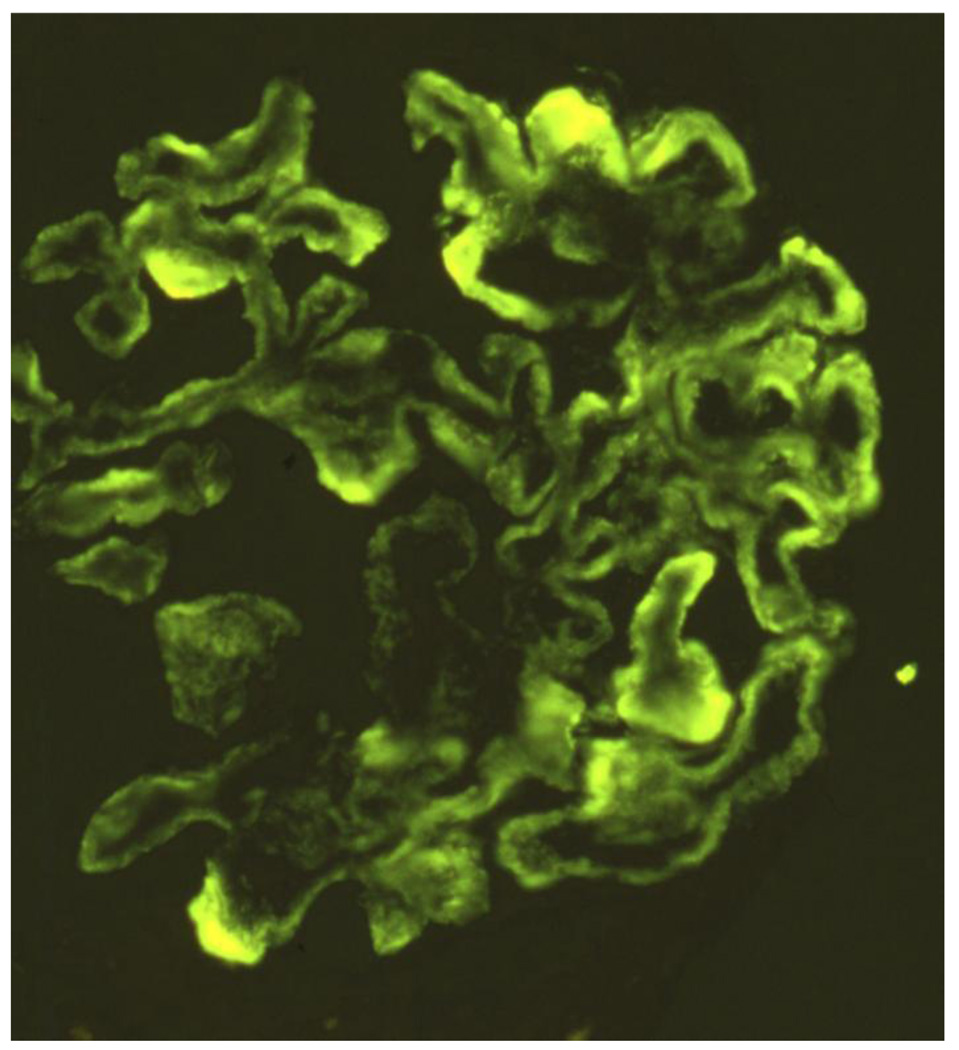
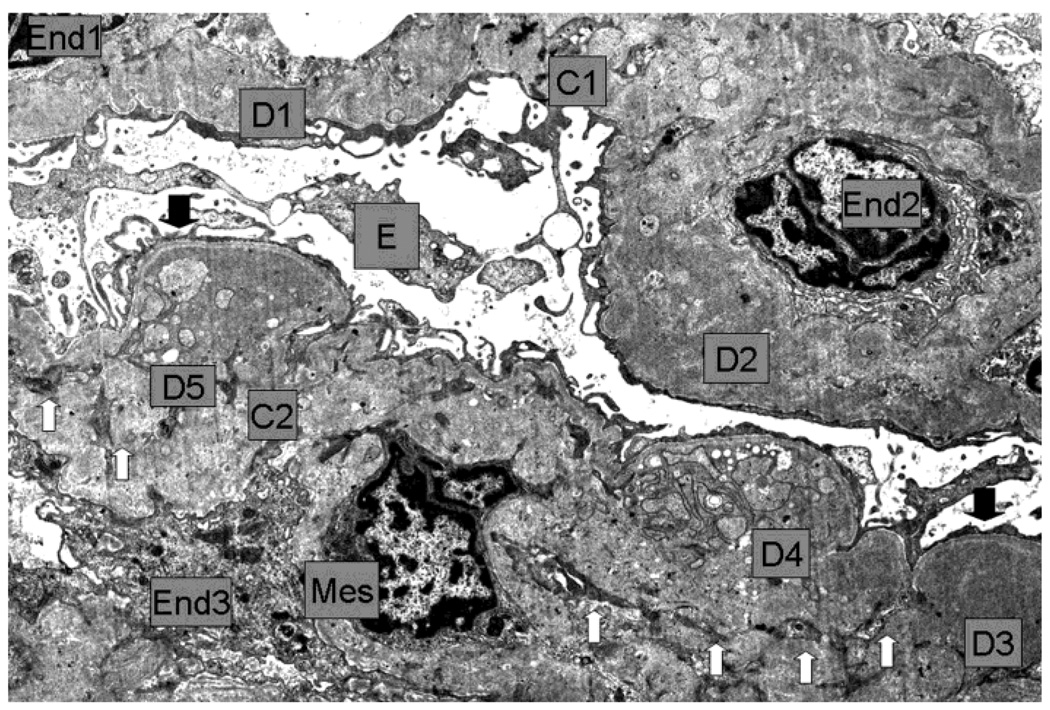
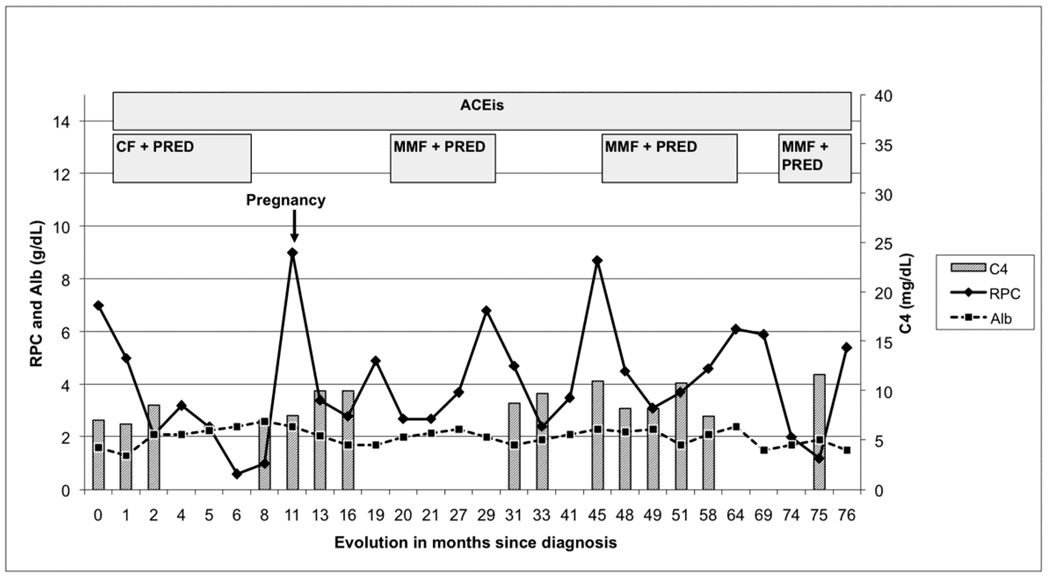
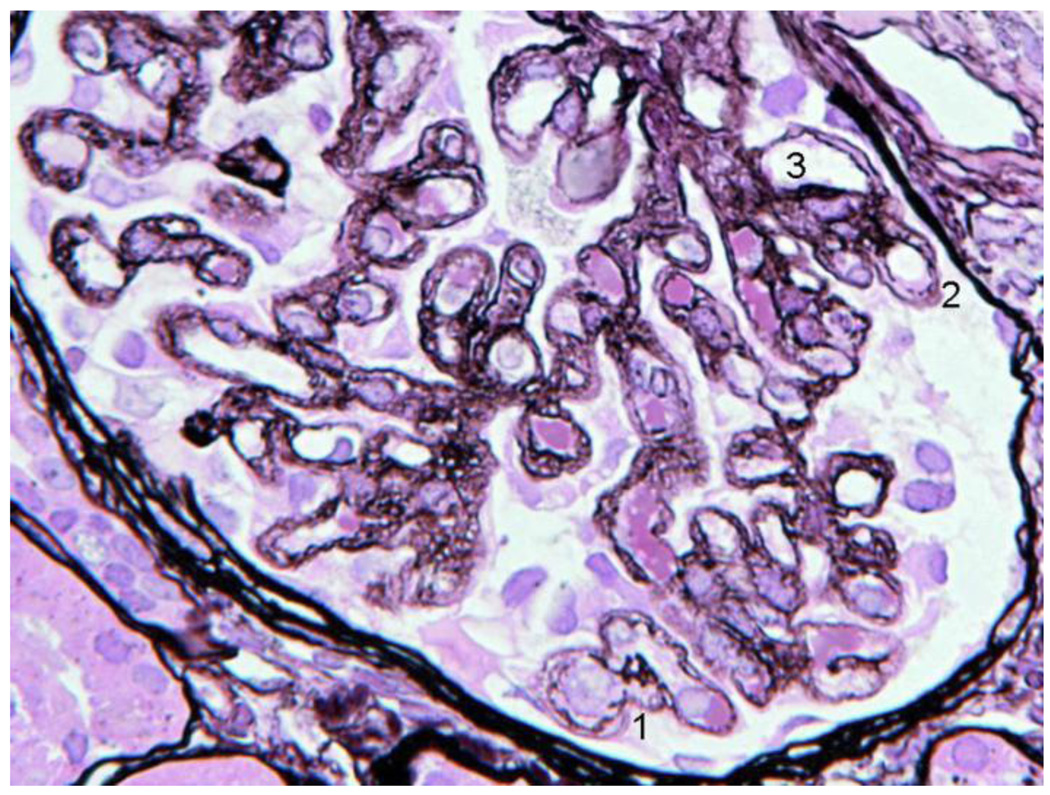
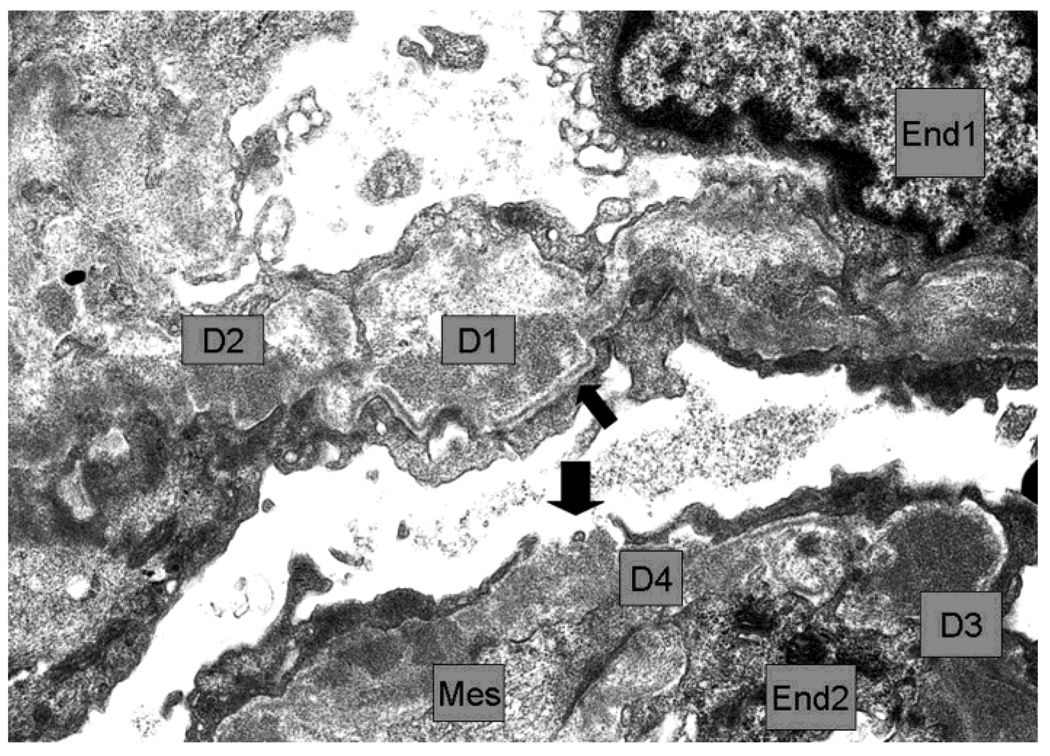
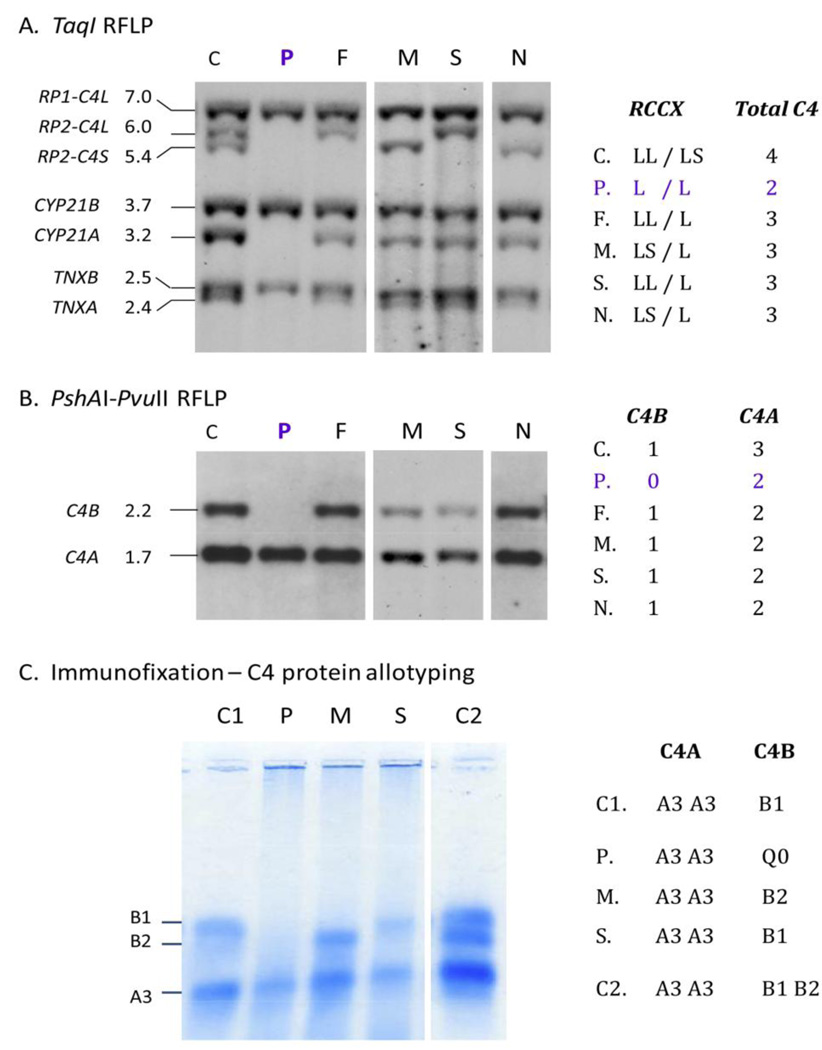
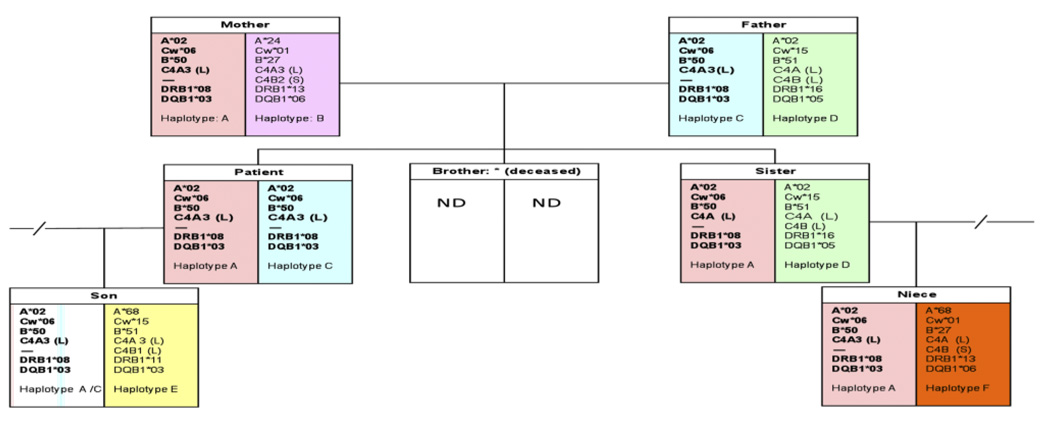
Homozygous complement C4B deficiency is described in a Southern European young female patient with Membranoproliferative Glomerulonephritis (MPGN) type III characterized by renal biopsies with strong complement C4 and IgG deposits. Low C4 levels were independent of clinical evolution or type of immunosuppression and were found in three other family members without renal disease or infections. HLA typing revealed that the patient has homozygous A*02, Cw*06, B*50 at the class I region, and DRB1*08 and DQB1*03 at the class II region. Genotypic and phenotypic studies demonstrated that the patient has homozygous monomodular RCCX in the HLA class III region, with single long C4A genes coding for C4A3 and complete C4B deficiency. Her father, mother, son and niece have heterozygous C4B deficiency. The patient's deceased brother had a history of Henoch-Schönlein Purpura (HSP), an immune complex-mediated proliferative glomerulonephritis. These findings challenge the putative pathophysiological roles of C4A and C4B and underscore the need to perform functional assays, C4 allotyping and genotyping on patients with persistently low serum levels of a classical pathway complement component and glomerulopathy associated with immune deposits.
Copyright © 2010 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Deficiencies of human complement component C4A and C4B and heterozygosity in length variants of RP-C4-CYP21-TNX (RCCX) modules in caucasians. The load of RCCX genetic diversity on major histocompatibility complex-associated disease.J Exp Med. 2000 Jun 19;191(12):2183-96. doi: 10.1084/jem.191.12.2183. J Exp Med. 2000. PMID: 10859342 Free PMC article.
-
Complete complement components C4A and C4B deficiencies in human kidney diseases and systemic lupus erythematosus.J Immunol. 2004 Aug 15;173(4):2803-14. doi: 10.4049/jimmunol.173.4.2803. J Immunol. 2004. PMID: 15294999
-
Sensitive and specific real-time polymerase chain reaction assays to accurately determine copy number variations (CNVs) of human complement C4A, C4B, C4-long, C4-short, and RCCX modules: elucidation of C4 CNVs in 50 consanguineous subjects with defined HLA genotypes.J Immunol. 2007 Sep 1;179(5):3012-25. doi: 10.4049/jimmunol.179.5.3012. J Immunol. 2007. PMID: 17709516
-
Genetic, structural and functional diversities of human complement components C4A and C4B and their mouse homologues, Slp and C4.Int Immunopharmacol. 2001 Mar;1(3):365-92. doi: 10.1016/s1567-5769(01)00019-4. Int Immunopharmacol. 2001. PMID: 11367523 Review.
-
Inherited deficiency of the fourth component of human complement.Immunodefic Rev. 1988;1(1):3-22. Immunodefic Rev. 1988. PMID: 3078708 Review.
Cited by
-
Screening and Analysis of Serum Protein Biomarkers Infected by Coronavirus Disease 2019 (COVID-19).Trop Med Infect Dis. 2022 Nov 25;7(12):397. doi: 10.3390/tropicalmed7120397. Trop Med Infect Dis. 2022. PMID: 36548652 Free PMC article.
-
Clinical features of patients with homozygous complement C4A or C4B deficiency.PLoS One. 2018 Jun 21;13(6):e0199305. doi: 10.1371/journal.pone.0199305. eCollection 2018. PLoS One. 2018. PMID: 29928053 Free PMC article.
-
Complement regulation and kidney diseases: recent knowledge of the double-edged roles of complement activation in nephrology.Clin Exp Nephrol. 2018 Feb;22(1):3-14. doi: 10.1007/s10157-017-1405-x. Epub 2017 Mar 24. Clin Exp Nephrol. 2018. PMID: 28341889 Review.
-
Medical Records-Based Genetic Studies of the Complement System.J Am Soc Nephrol. 2021 Aug;32(8):2031-2047. doi: 10.1681/ASN.2020091371. Epub 2021 May 3. J Am Soc Nephrol. 2021. PMID: 33941608 Free PMC article.
-
Genetically determined partial complement C4 deficiency states are not independent risk factors for SLE in UK and Spanish populations.Am J Hum Genet. 2012 Mar 9;90(3):445-56. doi: 10.1016/j.ajhg.2012.01.012. Epub 2012 Mar 1. Am J Hum Genet. 2012. PMID: 22387014 Free PMC article.
References
-
- Walport MJ. Complement-part I. New Engl. J. Med. 2001;344:1058–1066. - PubMed
-
- Chung EK, Wu YL, Yang Y, Zhou B, Yu CY. Human complement components C4A and C4B genetic diversities: complex genotypes and phenotypes. Curr. Protoc. Immunol. 2005:13.8.1–13.8.36. - PubMed
-
- Blanchong CA, Zhou B, Rupert KL, Chung EK, Jones KN, Sotos JF, Rennebohm RM, Yu CY. Deficiencies of human complement component C4A and C4B and heterozygosity in length variants of RP-C4-CYP21-TNX (RCCX) modules in Caucasians: the load of RCCX genetic diversity on MHC-associated disease. J. Exp. Med. 2000;191:2183–2196. - PMC - PubMed
-
- Yang Y, Chung EK, Wu YL, Savelli SL, Nagaraja HN, Zhou B, Hebert M, Jones KN, Shu Y, Kitzmiller K, Blanchong CA, McBride K, Higgins GC, Rennebohm RM, Rice RR, Hackshaw KV, Roubey RA, Grossman JM, Tsao BP, Birmingham DJ, Rovin BH, Hebert LA, Yu CY. Gene copy number variation and associated polymorphisms of complement component C4 in human systemic erythematosus (SLE): low copy number is a risk factor for and high copy number is a protective factor against European American SLE disease susceptibility. Am. J. Hum. Genet. 2007;80:1037–1054. - PMC - PubMed
-
- Yang Y, Chung EK, Zhou B, Lhotta K, Hebert LA, Birmingham DJ, Rovin BH, Yu CY. The intricate role of complement C4 in human systemic lupus erythematosus. Curr. Direct. Autoimmun. 2004;7:98–132. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
