

Somatic chromosome abnormalities in the lungs of patients with pulmonary arterial hypertension
- PMID: 20581168
- PMCID: PMC3001257
- DOI: 10.1164/rccm.201003-0491OC
Somatic chromosome abnormalities in the lungs of patients with pulmonary arterial hypertension
Abstract
Rationale: Vascular remodeling in pulmonary arterial hypertension (PAH) involves proliferation and migration of endothelial and smooth muscle cells, leading to obliterative vascular lesions. Previous studies have indicated that the endothelial cell proliferation is quasineoplastic, with evidence of monoclonality and instability of short DNA microsatellite sequences.
Objectives: To assess whether there is larger-scale genomic instability.
Methods: We performed genome-wide microarray copy number analysis on pulmonary artery endothelial cells and smooth muscle cells isolated from the lungs of patients with PAH.
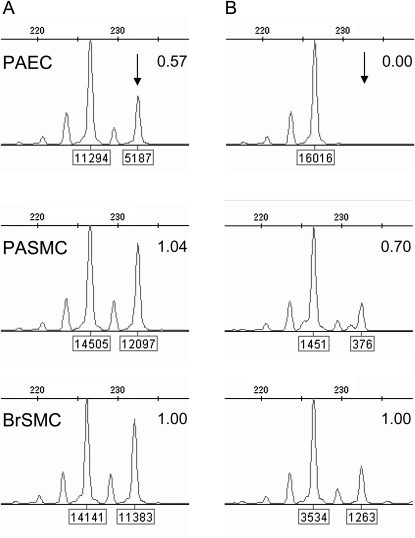
Measurements and main results: Mosaic chromosomal abnormalities were detected in PAEC cultures from five of nine PAH lungs but not in normal (n = 8) or disease control subjects (n = 5). Fluorescent in situ hybridization analysis confirmed the presence of these abnormalities in vivo in two of three cases. One patient harbored a germline mutation of BMPR2, the primary genetic cause of PAH, and somatic loss of chromosome-13, which constitutes a second hit in the same pathway by deleting Smad-8. In two female subjects with mosaic loss of the X chromosome, methylation analysis showed that the active X was deleted. One subject also showed completely skewed X-inactivation in the nondeleted cells, suggesting the pulmonary artery endothelial cell population was clonal before the acquisition of the chromosome abnormality.
Conclusions: Our data indicate a high frequency of genetically abnormal subclones within PAH lung vessels and provide the first definitive evidence of a second genetic hit in a patient with a germline BMPR2 mutation. We propose that these chromosome abnormalities may confer a growth advantage and thus contribute to the progression of PAH.
Figures


Comment in
-
Somatic mutations in pulmonary arterial hypertension: primary or secondary events?Am J Respir Crit Care Med. 2010 Nov 1;182(9):1094-6. doi: 10.1164/rccm.201007-1147ED. Am J Respir Crit Care Med. 2010. PMID: 21041561 No abstract available.
References
-
- Rubin LJ. Primary pulmonary hypertension. N Engl J Med 1997;336:111–117. - PubMed
-
- Gaine SP, Rubin LJ. Primary pulmonary hypertension. Lancet 1998;352:719–725. - PubMed
-
- Moncada S, Higgs EA. Prostaglandins in the pathogenesis and prevention of vascular disease. Blood Rev 1987;1:141–145. - PubMed
-
- Moncada S. Nitric oxide. J Hypertens Suppl 1994;12:S35–S39. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
