

Imatinib in pulmonary arterial hypertension patients with inadequate response to established therapy
- PMID: 20581169
- PMCID: PMC3001259
- DOI: 10.1164/rccm.201001-0123OC
Imatinib in pulmonary arterial hypertension patients with inadequate response to established therapy
Abstract
Rationale: Pulmonary arterial hypertension (PAH) is a progressive condition with a poor prognosis. Platelet-derived growth factor receptor (PDGFR) signaling plays an important role in its pathobiology.
Objectives: To assess safety, tolerability, and efficacy of the PDGFR inhibitor imatinib in patients with PAH.
Methods: Patients with PAH in functional classes II-IV were enrolled in a 24-week randomized, double-blind, placebo-controlled pilot study. Patients received imatinib (an inhibitor of PDGFR activity) 200 mg orally once daily (or placebo), which was increased to 400 mg if the initial dose was well tolerated. The primary endpoints were safety and change from baseline in the 6-minute-walk distance (6MWD). Secondary endpoints included hemodynamics and functional classification.
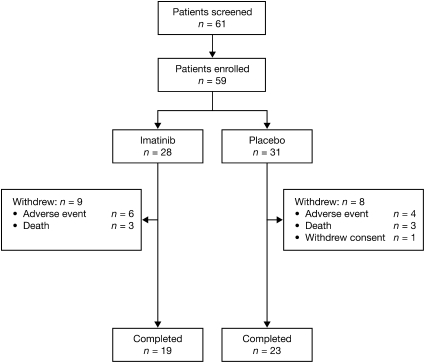
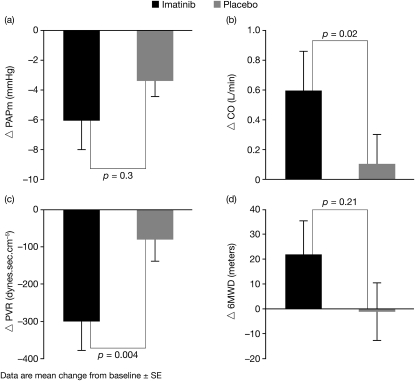
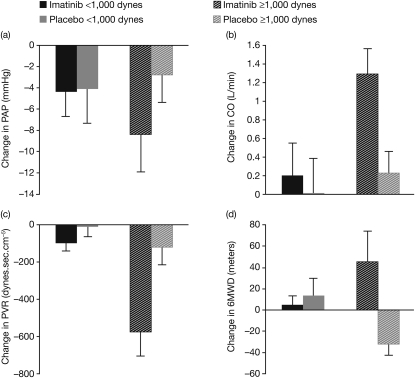
Measurements and main results: Fifty-nine patients enrolled (imatinib [n = 28]; placebo [n = 31]); 42 completed the study. Dropouts were equally matched between the two groups. In the intention-to-treat (ITT) population there was no significant change in the 6MWD (mean ± SD) in the imatinib versus placebo group (+22 ± 63 versus -1.0 ± 53 m). There was a significant decrease in pulmonary vascular resistance (imatinib -300 ± 347 versus placebo -78 ± 269 dynes · s · cm⁻⁵, P < 0.01) and increase in cardiac output (imatinib +0.6 ± 1.2 versus placebo -0.1 ± 0.9 L/min, P = 0.02). Serious adverse events occurred in 11 imatinib recipients (39%) and 7 placebo recipients (23%). Three deaths occurred in each group. Post hoc subgroup analyses suggest that patients with greater hemodynamic impairment may respond better than patients with less impairment.
Conclusions: These data from a Phase II study are consistent with imatinib being well tolerated in patients with PAH, and provide proof of concept for further studies evaluating its safety, tolerability, and efficacy in PAH. Clinical trial registered with www.clinicaltrials.gov (NCT00477269).
Figures
References
-
- Badesch DB, Champion HC, Gomez Sanchez MA, Hoeper MM, Loyd JE, Manes A, McGoon M, Naeige R, Olschewski H, Oudiz RJ, et al. Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2009;54:55S–66S. - PubMed
-
- D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991;115:343–349. - PubMed
-
- Galiè N, Brundage BH, Ghofrani HA, Oudiz RJ, Simonneau G, Safdar Z, Shapiro S, White RJ, Chan M, Beardsworth A, et al. Tadalafil therapy for pulmonary arterial hypertension. Circulation 2009;119:2894–2903. - PubMed
-
- Ghofrani HA, Wilkins MW, Rich S. Uncertainties in the diagnosis and treatment of pulmonary arterial hypertension. Circulation 2008;118:1195–1201. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
