

Angiogenesis and nerve growth factor at the osteochondral junction in rheumatoid arthritis and osteoarthritis
- PMID: 20581375
- PMCID: PMC2936950
- DOI: 10.1093/rheumatology/keq188
Angiogenesis and nerve growth factor at the osteochondral junction in rheumatoid arthritis and osteoarthritis
Abstract
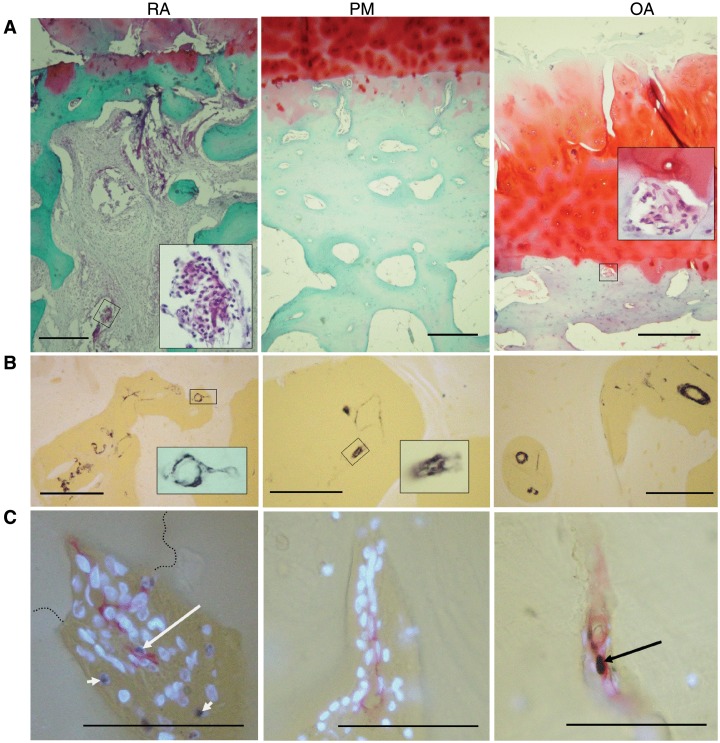
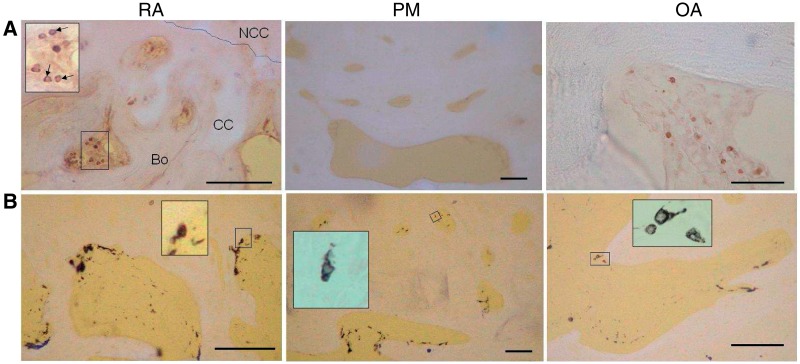
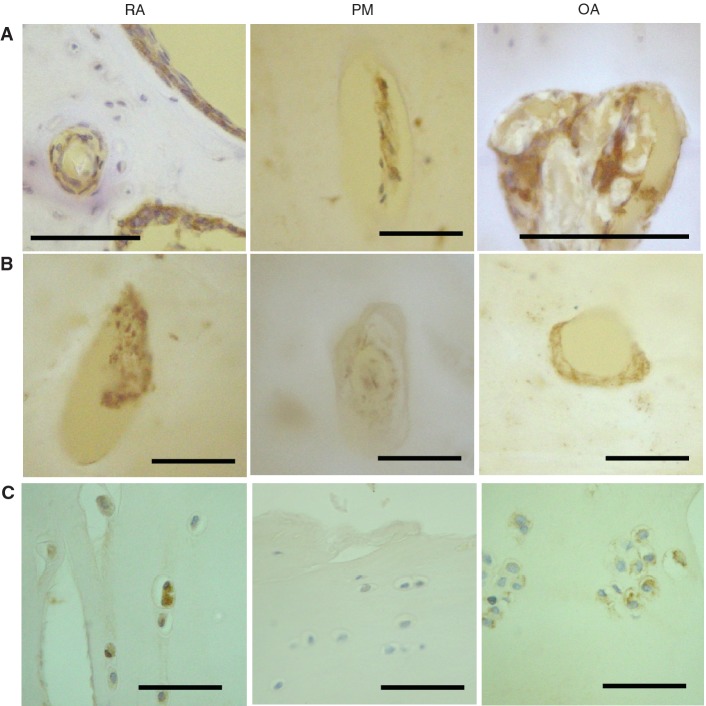
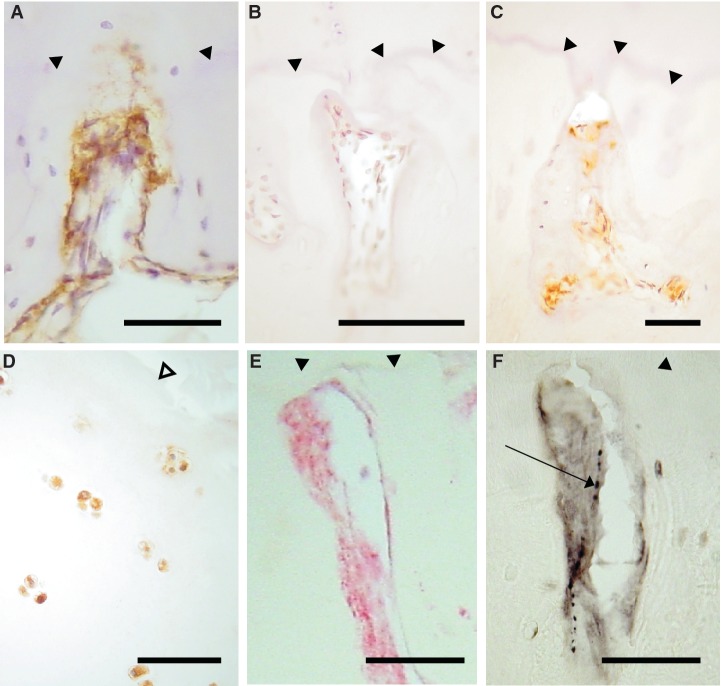
Objectives. The osteochondral junction can be a source of pain in both RA and OA. Growth of blood vessels and nerves from the subchondral bone into articular cartilage may mediate the association between joint pathology and symptoms. We have investigated associations between angiogenesis, inflammation and neurovascular growth factor expression at the osteochondral junction in human arthritis. Methods. Osteochondral junctions from medial tibial plateaux of patients undergoing arthroplasty for RA (n = 10) or OA (n = 11), or from non-arthritic post-mortem controls (n = 11) were characterized by immunohistochemistry for CD34 and smooth muscle α-actin (blood vessels), CD68 (macrophages), CD3 (lymphocytes), proliferating cell nuclear antigen, vascular endothelial, platelet-derived and nerve growth factor (NGF). Results. Osteochondral angiogenesis was demonstrated as increased endothelial cell proliferation and vascular density in non-calcified articular cartilage, both in RA and OA. Osteochondral angiogenesis was associated with subchondral bone marrow replacement by fibrovascular tissue expressing VEGF, and with increased NGF expression within vascular channels. RA was characterized by greater lymphocyte infiltration and PDGF expression than OA, whereas chondrocyte expression of VEGF was a particular feature of OA. NGF was observed in vascular channels that contained calcitonin gene-related peptide-immunoreactive sensory nerve fibres. Conclusions. Osteochondral angiogenesis in RA and OA is associated with growth factor expression by cells within subchondral spaces, vascular channels and by chondrocytes. NGF expression and sensory nerve growth may link osteochondral angiogenesis to pain in arthritis.
Figures
References
-
- Appel H, Kuhne M, Spiekermann S, et al. Immunohistochemical analysis of hip arthritis in ankylosing spondylitis: evaluation of the bone-cartilage interface and subchondral bone marrow. Arthritis Rheum. 2006;54:1805–13. - PubMed
-
- Bugatti S, Caporali R, Manzo A, Vitolo B, Pitzalis C, Montecucco C. Involvement of subchondral bone marrow in rheumatoid arthritis: lymphoid neogenesis and in situ relationship to subchondral bone marrow osteoclast recruitment. Arthritis Rheum. 2005;52:3448–59. - PubMed
-
- Kaneko M, Tomita T, Nakase T, et al. Expression of proteinases and inflammatory cytokines in subchondral bone regions in the destructive joint of rheumatoid arthritis. Rheumatology. 2001;40:247–55. - PubMed
-
- Lisignoli G, Piacentini A, Cristino S, et al. CCL20 chemokine induces both osteoblast proliferation and osteoclast differentiation: increased levels of CCL20 are expressed in subchondral bone tissue of rheumatoid arthritis patients. J Cell Physiol. 2007;210:798–806. - PubMed
-
- Burr DB, Schaffler MB. The involvement of subchondral mineralized tissues in osteoarthrosis: quantitative microscopic evidence. Microsc Res Tech. 1997;37:343–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
