

Single maintenance and reliever therapy (SMART) of asthma: a critical appraisal
- PMID: 20581409
- PMCID: PMC2975956
- DOI: 10.1136/thx.2009.128504
Single maintenance and reliever therapy (SMART) of asthma: a critical appraisal
Abstract
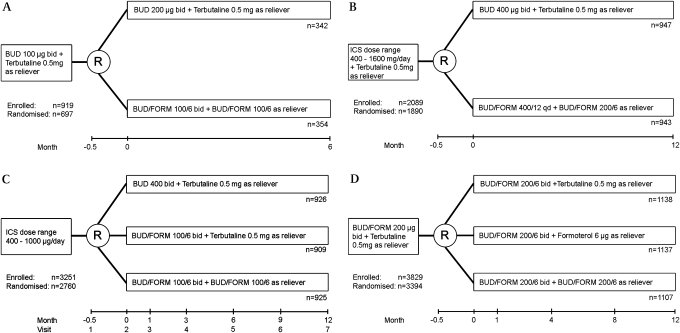
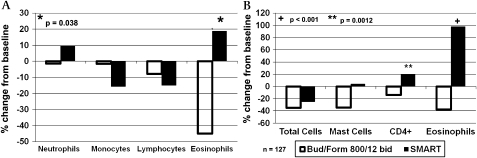
The use of a combination inhaler containing budesonide and formoterol as both maintenance and quick relief therapy (SMART) has been recommended as an improved method of using inhaled corticosteroid/long-acting beta agonist (ICS/LABA) therapy. Published double-blind trials show that budesonide/formoterol therapy delivered in SMART fashion achieves better asthma outcomes than budesonide monotherapy or lower doses of budesonide/formoterol therapy delivered in constant dosage. Attempts to compare budesonide/formoterol SMART therapy with regular combination ICS/LABA dosing using other compounds have been confounded by a lack of blinding and unspecified dose adjustment strategies. The asthma control outcomes in SMART-treated patients are poor; it has been reported that only 17.1% of SMART-treated patients are controlled. In seven trials of 6-12 months duration, patients using SMART have used quick reliever daily (weighted average 0.92 inhalations/day), have awakened with asthma symptoms once every 7-10 days (weighted average 11.5% of nights), have suffered asthma symptoms more than half of days (weighted average 54.0% of days) and have had a severe exacerbation rate of one in five patients per year (weighted average 0.22 severe exacerbations/patient/year). These poor outcomes may reflect the recruitment of a skewed patient population. Although improvement from baseline has been attributed to these patients receiving additional ICS therapy at pivotal times, electronic monitoring has not been used to test this hypothesis nor the equally plausible hypothesis that patients who are non-compliant with maintenance medication have used budesonide/formoterol as needed for self-treatment of exacerbations. Although the long-term consequences of SMART therapy have not been studied, its use over 1 year has been associated with significant increases in sputum and biopsy eosinophilia. At present, there is no evidence that better asthma treatment outcomes can be obtained by moment-to-moment symptom-driven use of ICS/LABA therapy than conventional physician-monitored and adjusted ICS/LABA therapy.
Conflict of interest statement
Figures
Comment in
-
Correspondence in relation to critical appraisal by Chapman et al.Thorax. 2011 Jan;66(1):86; discussion 87-8. doi: 10.1136/thx.2010.149633. Epub 2010 Nov 19. Thorax. 2011. PMID: 21097535 No abstract available.
-
Single maintenance and reliever therapy.Thorax. 2011 Jan;66(1):87; discussion 87-8. doi: 10.1136/thx.2010.150219. Epub 2010 Nov 19. Thorax. 2011. PMID: 21097537 No abstract available.
-
Single maintenance and reliever therapy (SMART) of asthma.Thorax. 2011 Jan;66(1):86-7; discussion 87-8. doi: 10.1136/thx.2010.149773. Epub 2010 Nov 19. Thorax. 2011. PMID: 21097538 No abstract available.
References
-
- Global Initiative for Asthma (GINA) Global strategy for asthma management and prevention. http://www.ginasthma.com (accessed 9 Dec 2008).
-
- Greening AP, Ind PW, Northfield M, et al. Added salmeterol versus higher-dose corticosteroid in asthma patients with symptoms on existing inhaled corticosteroid. Lancet 1994;344:219–24 - PubMed
-
- Pauwels RA, Lofdahl CG, Postma DS, et al. ; Formoterol and Corticosteroids Establishing Therapy (FACET) International Study Group Effect of inhaled formoterol and budesonide on exacerbations of asthma. N Engl J Med 1997;337:1405–11 - PubMed
-
- Bateman ED, Boushey HA, Bousquet J, et al. Can guideline-defined asthma control be achieved? The Gaining Optimal Asthma Control study. Am J Respir Crit Care Med 2004;170:836–44 - PubMed