

Why treat insomnia?
- PMID: 20582296
- PMCID: PMC2882812
- DOI: 10.4088/PCC.08r00743bro
Why treat insomnia?
Abstract
Objective: To make the case that insomnia is better conceptualized, not as a symptom, but as a primary disorder.
Data sources: PubMed was searched from 1975-2009 using the search terms insomnia, insomnia and treatment, insomnia and cost, and insomnia and treatment and safety.
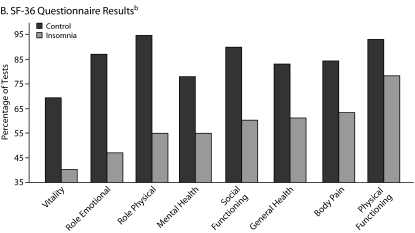
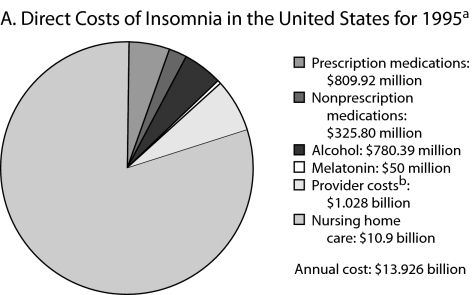
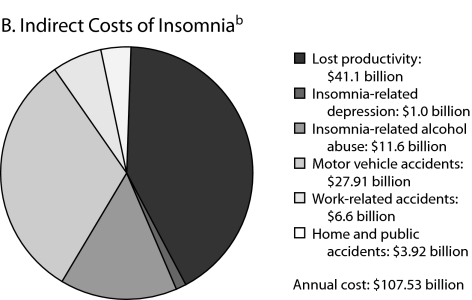
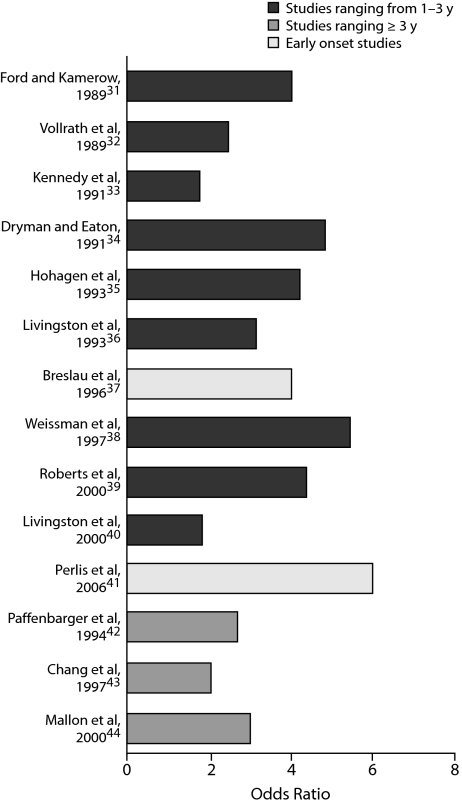
Study selection: English-language articles and other materials were selected to address the following claims: insomnia is unremitting, insomnia is disabling, insomnia is costly, insomnia is pervasive, insomnia is pernicious, and insomnia treatment is safe and effective.
Data extraction/synthesis: Insomnia, at least when chronic, should be conceptualized as a comorbid condition, one for which effective interventions are available.
Conclusions: It is speculated that treatment for insomnia will only become the norm when it has been demonstrated that treatment not only addresses the problem of insomnia but also serves to reduce medical and psychiatric morbidity. At that time, the question will no longer be "Why treat insomnia?" but instead "When isn't insomnia treatment indicated?"
Figures
References
-
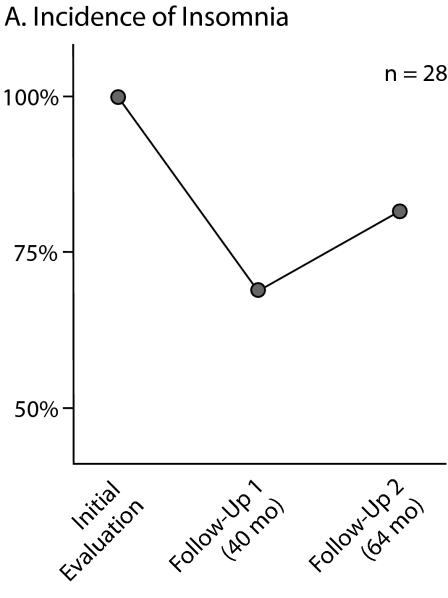
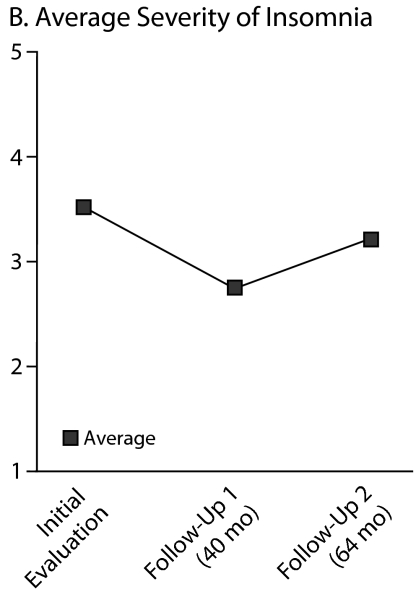
- Mendelson WB. Long-term follow-up of chronic insomnia. Sleep. 1995;18(8):698–701. - PubMed
-
- Morin CM, Belanger L, LeBlanc M, et al. The natural history of insomnia: a population-based, 3-year, longitudinal study. Arch Intern Med. 2009;169(5):447–453. - PubMed
-
- Young TB. Natural history of chronic insomnia. J Clin Sleep Med. 2005;1:e466–e467.
-
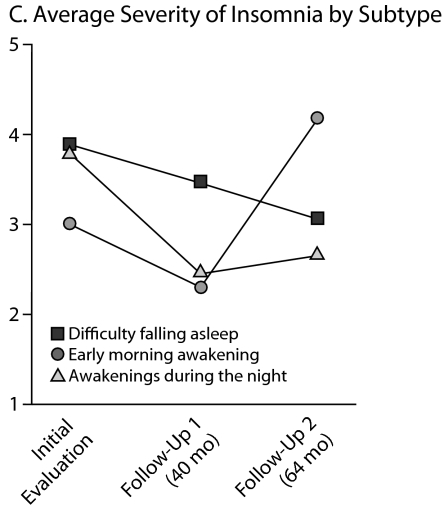
- Hohagen F, Kappler C, Schramm E, et al. Sleep onset insomnia, sleep maintaining insomnia and insomnia with early morning awakening: temporal stability of subtypes in a longitudinal study on general practice attenders. Sleep. 1994;17(6):551–554. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources