

Routine ultrasound and limited computed tomography for the diagnosis of acute appendicitis
- PMID: 20582544
- PMCID: PMC2936677
- DOI: 10.1007/s00268-010-0694-y
Routine ultrasound and limited computed tomography for the diagnosis of acute appendicitis
Abstract
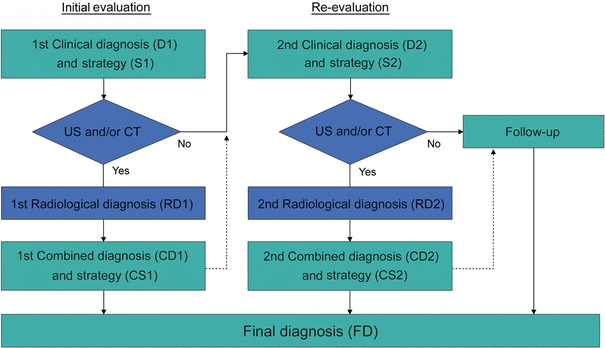
Background: Acute appendicitis continues to be a challenging diagnosis. Preoperative radiological imaging using ultrasound (US) or computed tomography (CT) has gained popularity as it may offer a more accurate diagnosis than classic clinical evaluation. The optimal implementation of these diagnostic modalities has yet to be established. The aim of the present study was to investigate a diagnostic pathway that uses routine US, limited CT, and clinical re-evaluation for patients with acute appendicitis.
Methods: A prospective analysis was performed of all patients presenting with acute abdominal pain at the emergency department from June 2005 until July 2006 using a structured diagnosis and management flowchart. Daily practice was mimicked, while ensuring a valid assessment of clinical and radiological diagnostic accuracies and the effect they had on patient management.
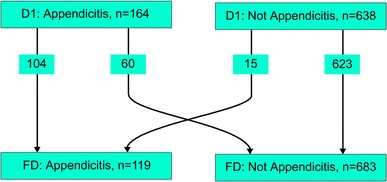
Results: A total of 802 patients were included in this analysis. Additional radiological imaging was performed in 96.3% of patients with suspected appendicitis (n = 164). Use of CT was kept to a minimum (17.9%), with a US:CT ratio of approximately 6:1. Positive and negative predictive values for the clinical diagnosis of appendicitis were 63 and 98%, respectively; for US 94 and 97%, respectively; and for CT 100 and 100%, respectively. The negative appendicitis rate was 3.3%, the perforation rate was 23.5%, and the missed perforated appendicitis rate was 3.4%. No (diagnostic) laparoscopies were performed.
Conclusions: A diagnostic pathway using routine US, limited CT, and clinical re-evaluation for patients with acute abdominal pain can provide excellent results for the diagnosis and treatment of appendicitis.
Figures
Comment in
-
Re: Routine ultrasound and limited computed tomography for the diagnosis acute appendicitis. Editor's note.World J Surg. 2011 Feb;35(2):294. doi: 10.1007/s00268-010-0852-2. World J Surg. 2011. PMID: 21086126 No abstract available.
-
Routine ultrasound and limited computed tomography for the diagnosis of acute appendicitis: a surgeon's perspective.World J Surg. 2011 Feb;35(2):295-6. doi: 10.1007/s00268-010-0866-9. World J Surg. 2011. PMID: 21125273 No abstract available.
References
-
- Velanovich V, Satava R. Balancing the normal appendectomy rate with the perforated appendicitis rate: implications for quality assurance. Am Surg. 1992;58:264–269. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
