

Dural tears in percutaneous endoscopic lumbar discectomy
- PMID: 20582555
- PMCID: PMC3036033
- DOI: 10.1007/s00586-010-1493-8
Dural tears in percutaneous endoscopic lumbar discectomy
Abstract
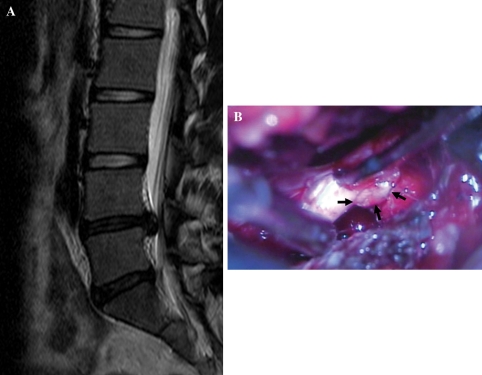
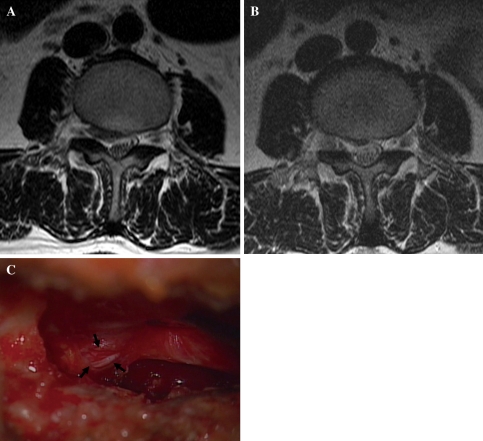
The objective of the study was to demonstrate the clinical characteristics of dural tears during percutaneous endoscopic lumbar discectomy (PELD) and to discuss how to prevent this unintended complication. The study used data from 816 consecutive patients who underwent PELD between 2003 and 2007. A total of nine patients (1.1%) experienced symptomatic dural tears. The clinical outcomes were evaluated using the visual analogue scale (VAS), the Oswestry disability index (ODI), and modified MacNab criteria. Intractable radicular pain was the most common symptom, while classical manifestations, such as CSF leakage or wound swelling, were rare. In three of the nine cases, the dural tears were detected intraoperatively, while the remaining six cases were not recognized during the procedure. Among the unrecognized patients, two patients were found with nerve root herniation causing profound neurological deficits. All patients were managed by secondary open repair surgeries. The mean follow-up period was 30.8 months. The mean VAS of radicular leg pain improved from 8.3 to 2.6, and that of back pain improved from 4.1 to 2.6. The mean ODI improved from 69.6 to 29.2%. The final outcomes were excellent in one, good in five, fair in one, and poor in two patients. As application of the endoscopic procedure has been broadened to more complex cases, the risk of dural tears may increase. Unrecognized dural tear with nerve root herniation may cause permanent neurological sequelae. Accurate information and proper technical considerations are essential to prevent this unpredictable complication.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
