

Does delay in diagnosing colorectal cancer in symptomatic patients affect tumor stage and survival? A population-based observational study
- PMID: 20584274
- PMCID: PMC2907342
- DOI: 10.1186/1471-2407-10-332
Does delay in diagnosing colorectal cancer in symptomatic patients affect tumor stage and survival? A population-based observational study
Abstract
Background: Diagnosing colorectal cancer (CRC) at an early stage improves survival. To what extent any delay affects outcome once patients are symptomatic is still unclear.Our objectives were to evaluate the association between diagnostic delay and survival in symptomatic patients with early stage CRC and late stage CRC.
Methods: Prospective population-based observational study evaluating daily clinical practice in Northern Holland. Diagnostic delay was determined through questionnaire-interviews. Dukes' stage was classified into two groups: early stage (Dukes A or B) and late stage (Dukes C or D) cancer. Patients were followed up for 3.5 years after diagnosis.
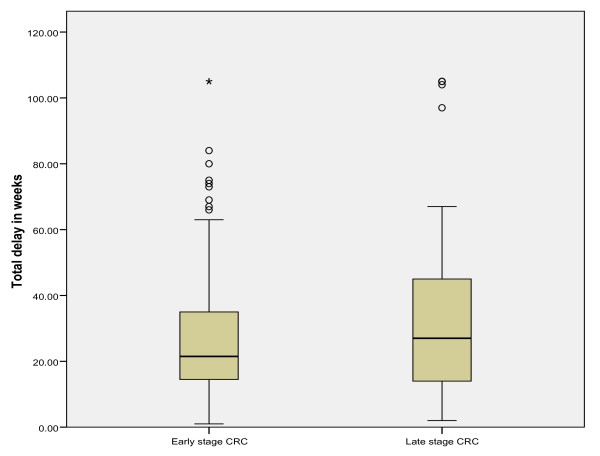
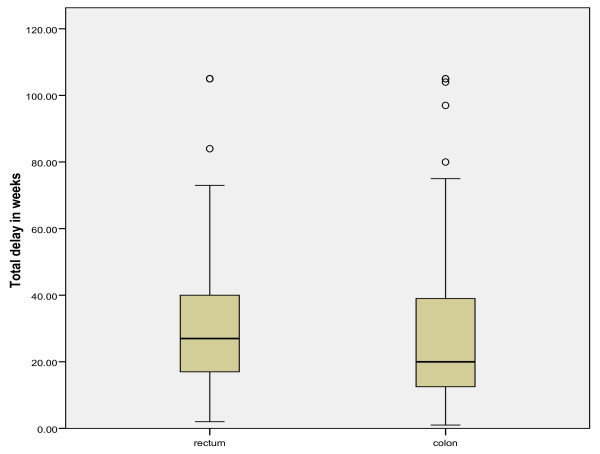
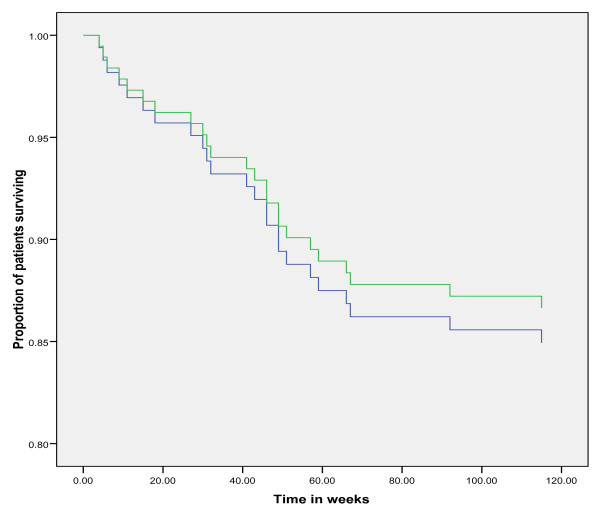
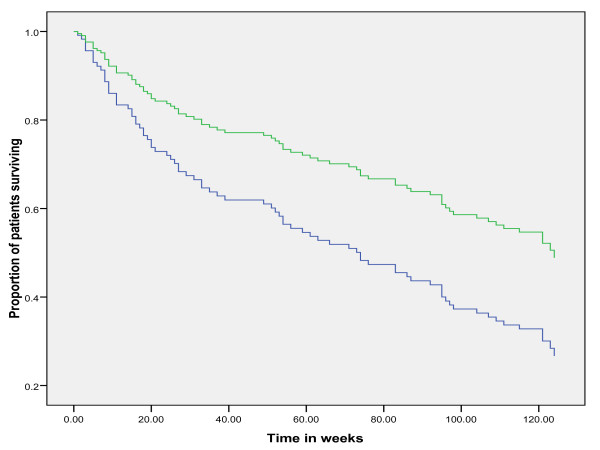
Results: In total, 272 patients were available for analysis. Early stage CRC was present in 136 patients while 136 patients had late stage CRC. The mean total diagnostic delay (SE) was 31 (1.5) weeks in all CRC patients. No significant difference was observed in the mean total diagnostic delay in early versus late stage CRC (p = 0.27).In early stage CRC, no difference in survival was observed between patients with total diagnostic delay shorter and longer than the median (Kaplan-Meier, log-rank p = 0.93).In late stage CRC, patients with a diagnostic delay shorter than the median had a shorter survival than patients with a diagnostic delay longer than the median (log-rank p = 0.01). In the multivariate Cox regression model with survival as dependent variable and median delay, age, open access endoscopy, number and type of symptoms as independent variables, the odd's ratio for survival in patients with long delay (>median) versus short delay (</=median) was 1.8 (95% confidence interval (CI) 1.1 to 3.0; p = 0.01). Tumor-site was not associated with patient survival. When separating late stage CRC in Dukes C and Dukes D tumors, a shorter delay was associated with a shorter survival in Dukes D tumors only and not in Dukes C tumors.
Conclusion: In symptomatic CRC patients, a longer diagnostic and therapeutic delay in routine clinical practice was not associated with an adverse effect on survival. The time to CRC diagnosis and initiation of treatment did not differ between early stage and late stage colorectal cancer.
Figures
Similar articles
-
Multivariate analysis of the prognostic value of CEA and CA 19-9 serum levels in colorectal cancer.Anticancer Res. 2000 Nov-Dec;20(6D):5195-8. Anticancer Res. 2000. PMID: 11326694
-
Clinical significance of circulating tumor cells, including cancer stem-like cells, in peripheral blood for recurrence and prognosis in patients with Dukes' stage B and C colorectal cancer.J Clin Oncol. 2011 Apr 20;29(12):1547-55. doi: 10.1200/JCO.2010.30.5151. Epub 2011 Mar 21. J Clin Oncol. 2011. PMID: 21422427
-
For patients with Dukes' B (TNM Stage II) colorectal carcinoma, examination of six or fewer lymph nodes is related to poor prognosis.Cancer. 1998 Aug 15;83(4):666-72. Cancer. 1998. PMID: 9708929
-
Global Distribution of Colorectal Cancer Staging at Diagnosis: An Evidence Synthesis.Clin Gastroenterol Hepatol. 2024 Dec 16:S1542-3565(24)01104-2. doi: 10.1016/j.cgh.2024.11.019. Online ahead of print. Clin Gastroenterol Hepatol. 2024. PMID: 39694204 Review.
-
Impact of delay in diagnosis and treatment-initiation on disease stage and survival in oral cavity cancer: a systematic review.Acta Oncol. 2021 Sep;60(9):1083-1090. doi: 10.1080/0284186X.2021.1931712. Epub 2021 May 27. Acta Oncol. 2021. PMID: 34043480
Cited by
-
AGA Rapid Recommendations for Gastrointestinal Procedures During the COVID-19 Pandemic.Gastroenterology. 2020 Aug;159(2):739-758.e4. doi: 10.1053/j.gastro.2020.03.072. Epub 2020 Apr 1. Gastroenterology. 2020. PMID: 32247018 Free PMC article. Review. No abstract available.
-
Fall of another myth for colon cancer: Duration of symptoms does not differ between right- or left-sided colon cancers.Turk J Gastroenterol. 2019 Aug;30(8):686-694. doi: 10.5152/tjg.2019.17770. Turk J Gastroenterol. 2019. PMID: 31418412 Free PMC article.
-
Time from first presentation in primary care to treatment of symptomatic colorectal cancer: effect on disease stage and survival.Br J Cancer. 2014 Jul 29;111(3):461-9. doi: 10.1038/bjc.2014.352. Epub 2014 Jul 3. Br J Cancer. 2014. PMID: 24992583 Free PMC article.
-
A prospective study of the effect of bowel movement frequency, constipation, and laxative use on colorectal cancer risk.Am J Gastroenterol. 2014 Oct;109(10):1640-9. doi: 10.1038/ajg.2014.233. Epub 2014 Sep 16. Am J Gastroenterol. 2014. PMID: 25223576 Free PMC article.
-
Factors related with symptom duration until diagnosis and treatment of symptomatic colorectal cancer.BMC Cancer. 2013 Feb 23;13:87. doi: 10.1186/1471-2407-13-87. BMC Cancer. 2013. PMID: 23432789 Free PMC article.
References
-
- Ferlay J, Bray F, Pisani P, Parkin DM. GLOBOCAN 2000: cancer incidence, mortality and prevalence worldwide. IARC Press. Lyon; 2001.
-
- Sant M, Aareleid T, Berrino F, Bielska Lasota M, Carli PM, Faivre J, Grosclaude P, Hedelin G, Matsuda T, Moller H, Moller T, Verdecchia A, Capocaccia R, Gatta G, Micheli A, Santaquilani M, Roazzi P, Lisi D. EUROCARE Working Group. Eurocare-3: survival of cancer patients diagnosed 1990-94 - results and commentary. Ann Oncol. 2003;14(Suppl 5):v61–v118. doi: 10.1093/annonc/mdg754. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
