

Angiography and embolisation for solid abdominal organ injury in adults - a current perspective
- PMID: 20584325
- PMCID: PMC2907361
- DOI: 10.1186/1749-7922-5-18
Angiography and embolisation for solid abdominal organ injury in adults - a current perspective
Abstract
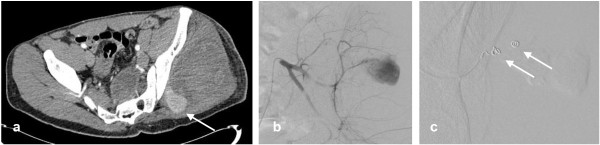
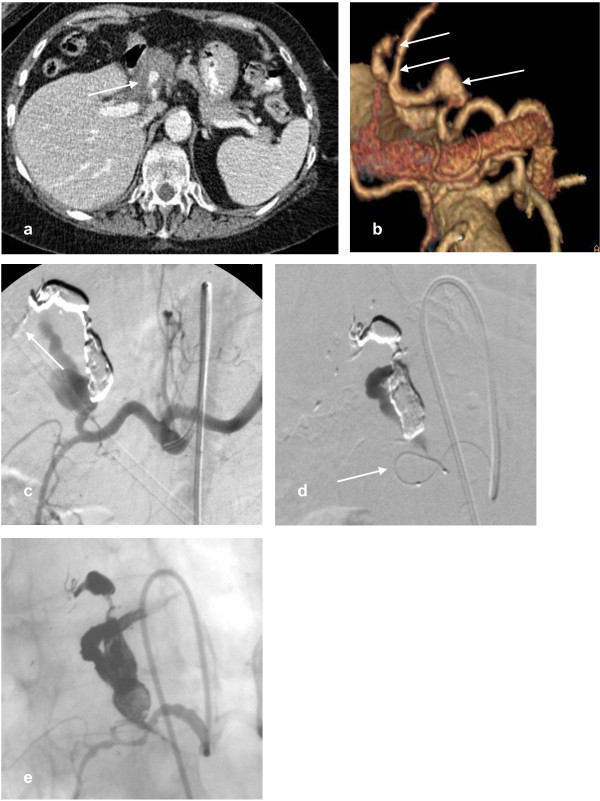
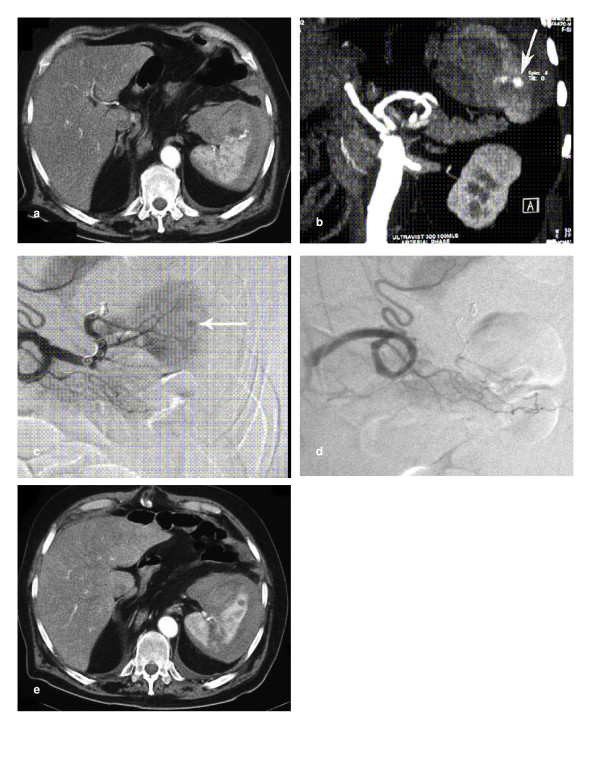
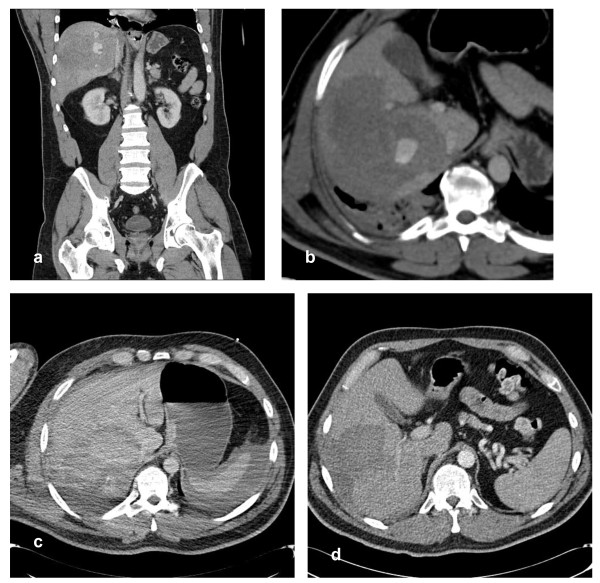
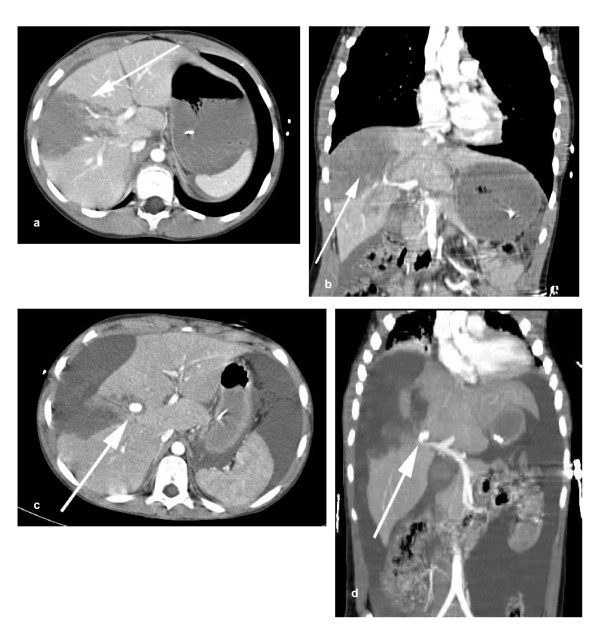
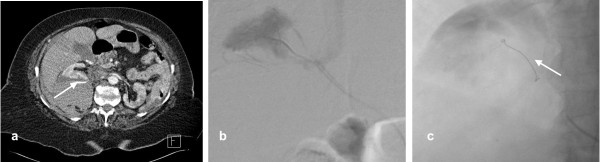
Over the past twenty years there has been a shift towards non-operative management (NOM) for haemodynamically stable patients with abdominal trauma. Embolisation can achieve haemostasis and salvage organs without the morbidity of surgery, and the development and refinement of embolisation techniques has widened the indications for NOM in the management of solid organ injury. Advances in computed tomography (CT) technology allow faster scanning times with improved image quality. These improvements mean that whilst surgery is still usually recommended for patients with penetrating injuries, multiple bleeding sites or haemodynamic instability, the indications for NOM are expanding.We present a current perspective on angiography and embolisation in adults with blunt and penetrating abdominal trauma with illustrative examples from our practice including technical advice.
Figures
References
-
- World Health Organisation. Guidelines for essential trauma care. 2004. http://whqlibdoc.who.int/publications/2004/9241546409.pdf
LinkOut - more resources
Full Text Sources
Miscellaneous
