

doi: 10.1177/15910199050110S117.
Epub 2005 Oct 27.
Basics and Principles in the Application of Onyx LD Liquid Embolic System in the Endovascular Treatment of Cerebral Arteriovenous Malformations
Affiliations
- PMID: 20584468
- PMCID: PMC3404755
- DOI: 10.1177/15910199050110S117
Item in Clipboard
Basics and Principles in the Application of Onyx LD Liquid Embolic System in the Endovascular Treatment of Cerebral Arteriovenous Malformations
Interv Neuroradiol.
.
No abstract available
Figures
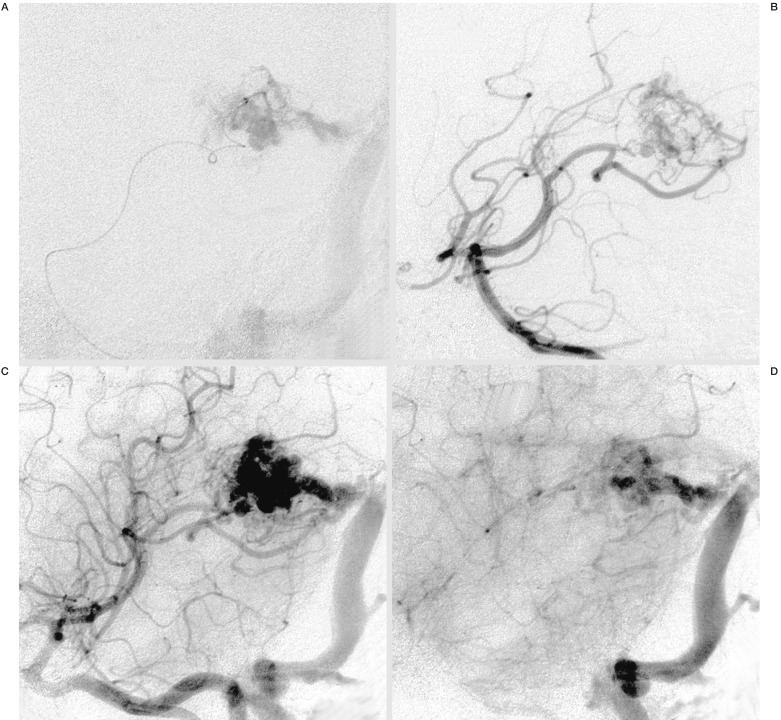
A) Intranidal positioning of the Microcatheter, Marathon™, in a small AVM of the left trigonum in an oblique projection and superselective injection of contrast media. B-D) Angiogram of the right vertebral artery in an early and later arterial (B,C) and venous phase (D) in the same projection, demonstrating the small arterial feeders and nidus with moderate flow and the main venous draining vein into the left sinus transversus.
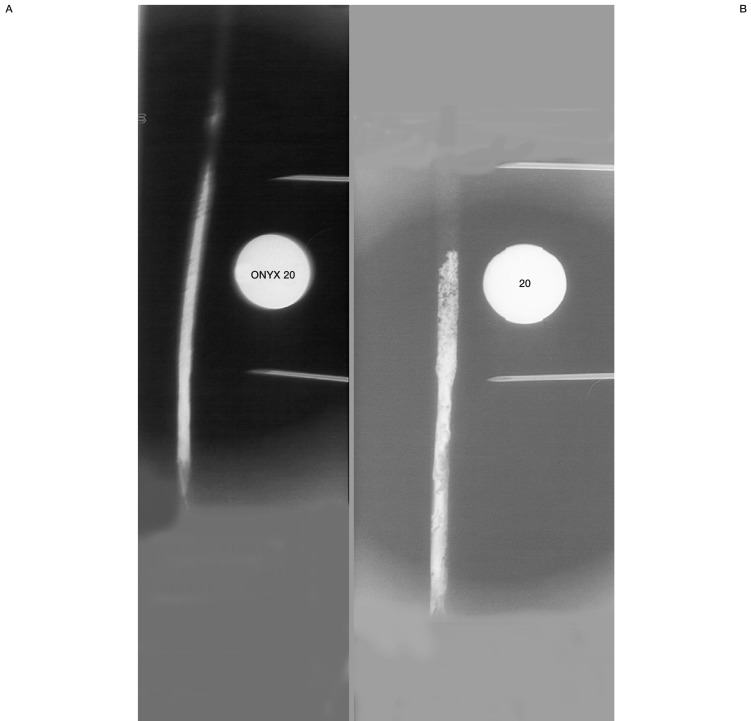
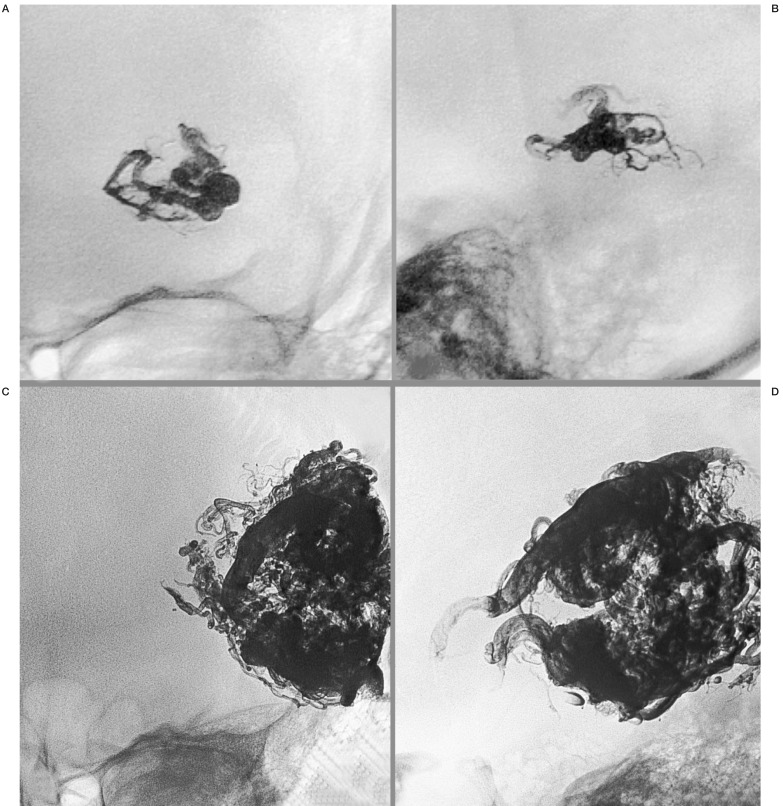
Results of Onyx 20 injection in a hydraulic pump model with a simulated arterial flow of 60 ml/min. The "nidus" is in a tube consisting of compressed foam and extends within the length marked by the needles (40 mm). A) "Intranidal" positioning of the Microcatheter, Ultraflow, in the proximal part of the foam with little reflux and homogenous filling of the entire "nidus". B) Postioning of the same microcatheter just below the level of the "nidus" with huge reflux and filling up only half of the foam.
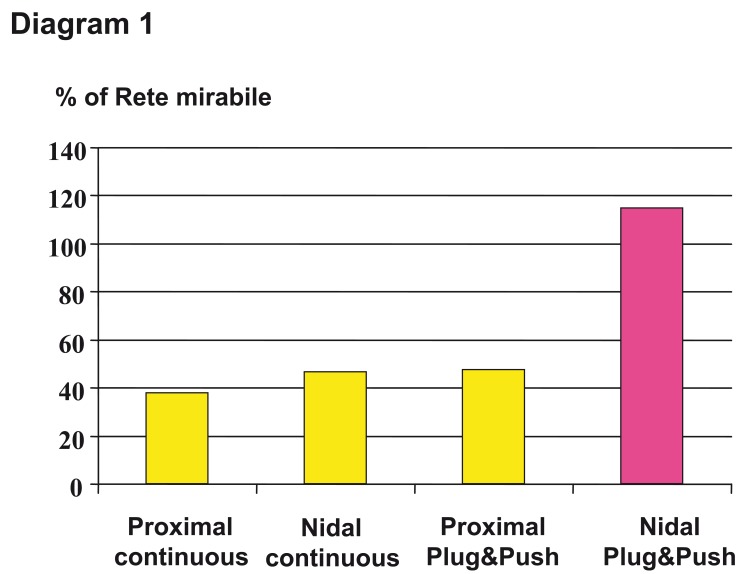
Results of different injection techniques (continuous versus plug&push technique) and microcatheter positions below (proximal) and within the "nidus" (nidal). Satisfactory result only after intranidal postioning and using the plug and push technique. The over one hundred percent filling in this experimental work using the rete mirabile of the swine as a biological AVM model is explained by ongoing further embolization of the contralateral part of the rete.
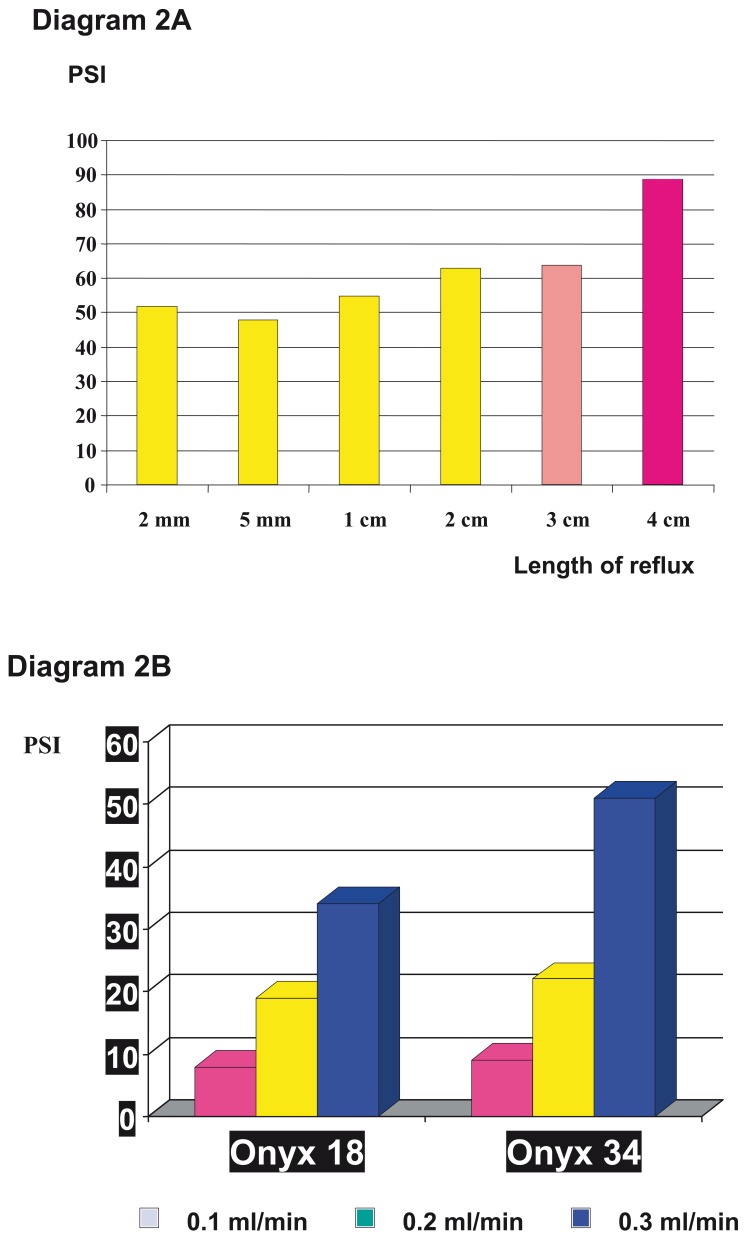
Demonstration of the increase of pressure inside the microcatheter A) after a length of reflux over 3 cm, B) and dependance on the injection speed and viscosity of Onyx.
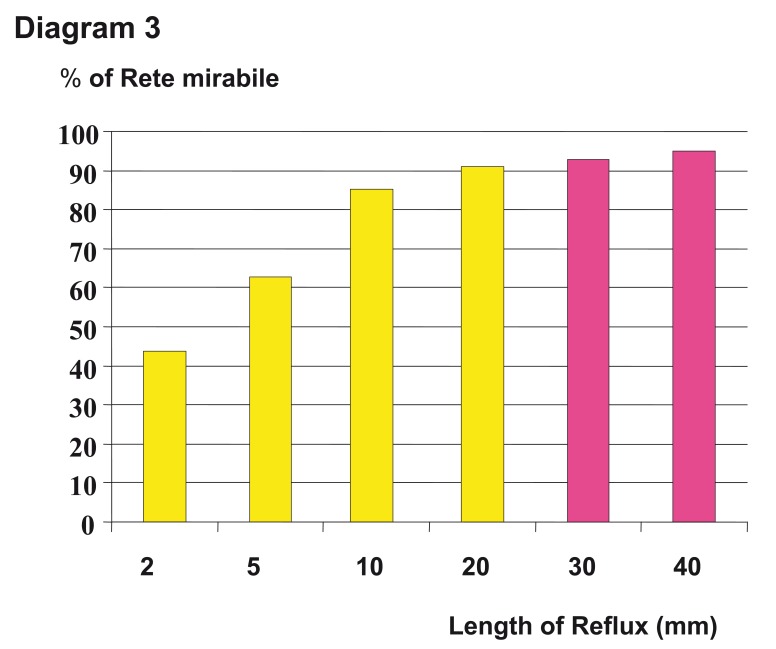
Different results of the filling of the rete mirabile in swine regarding the length of reflux. Beyond a length of 2 cm there is no significant increase of filling.
Two demonstrations of a homogeneous spongic cast after embolization of AVMS, both in ap and lateral projections. A) Same patient as in Figure 1. Cast after injection 0.9 ml of Onyx 20 after single catherization and 90% angiographic occlusion of the AVM. B) Another patient with a giant temporal AVM on the left side. Cast after injection of 26 ml of Onyx in five sessions using Onyx of different viscosities and 90% occlusion of the AVM. After embolization and surgical resection the patient was clinically asymptomatic.
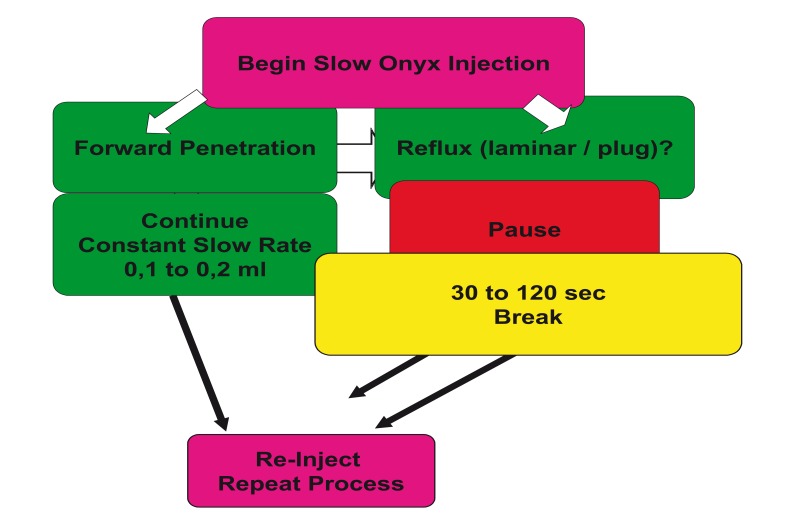
Summary and illustration of the decision process during the Onyx injection from the beginning of the application in repeat and reinject cycles.
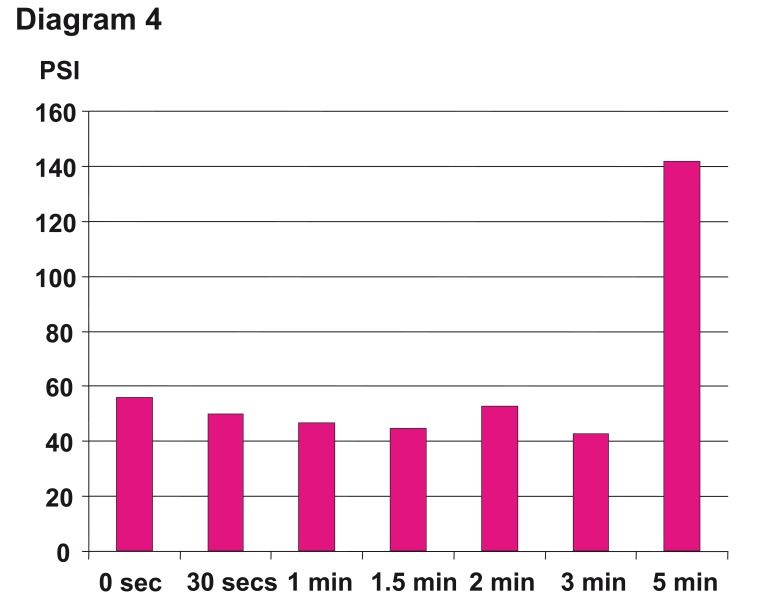
Different times of breaks (waiting time) after the Onyx injection period from zero to 5 minutes and the influence on the pressure inside the microcatheter clearly demonstrates that beyond 3 min, there is an immense increase of the pressure and with it risk of unintentional microcatheter occlusion. Two minutes maximum is recommended in the Instructions For Use.
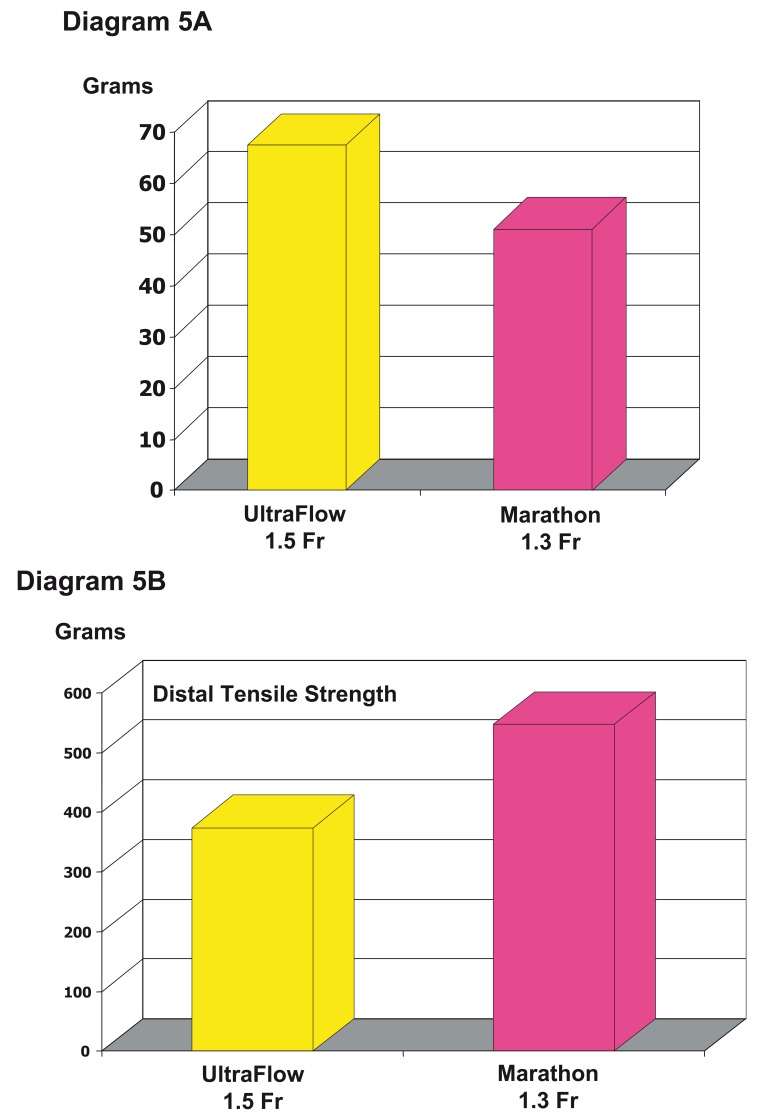
Differences between Ultraflow™ and Marathon™ regarding the soft and nitinol braided distal tip due to the detachment force (A) and the tensile strength (B). A) Comparison of the forces necessary to retrieve the microcatheters out of a cast with a reflux of 3 cm demonstrating that the detachment force in the braided one is 25% less. B) The distal tensile strength is one third greater in the braided one and demonstrates the increase stretch resistance of the distal, soft part of the microcatheter. This allows more tension to be brought to the tip and with it to pull out the catheter with more ease out of the cast.
Similar articles
-
Neurological morbidity and mortality associated with the endovascular treatment of cerebral arteriovenous malformations before and during the Onyx era.J Neurosurg. 2015 Jun;122(6):1492-7. doi: 10.3171/2015.2.JNS131368. Epub 2015 Mar 27. J Neurosurg. 2015. PMID: 25816081
-
Embolic Agents and Microcatheters for Endovascular Treatment of Cerebral Arteriovenous Malformations.World Neurosurg. 2020 Sep;141:383-388. doi: 10.1016/j.wneu.2020.06.118. Epub 2020 Jun 24. World Neurosurg. 2020. PMID: 32592963 Review.
-
Endovascular treatment of cerebral arteriovenous malformations with Onyx embolization.Chin Med J (Engl). 2005 Dec 20;118(24):2041-5. Chin Med J (Engl). 2005. PMID: 16438900
-
A prospective, multicenter, randomized trial of the Onyx liquid embolic system and N-butyl cyanoacrylate embolization of cerebral arteriovenous malformations. Clinical article.J Neurosurg. 2010 Oct;113(4):733-41. doi: 10.3171/2010.3.JNS09370. J Neurosurg. 2010. PMID: 20433277 Clinical Trial.
-
Onyx: a unique neuroembolic agent.Expert Rev Med Devices. 2006 Nov;3(6):705-15. doi: 10.1586/17434440.3.6.705. Expert Rev Med Devices. 2006. PMID: 17280535 Review.
Cited by
-
Transarterial embolization of the external carotid artery in the treatment of life-threatening haemorrhage following blunt maxillofacial trauma.Radiol Oncol. 2020 May 28;54(3):253-262. doi: 10.2478/raon-2020-0035. Radiol Oncol. 2020. PMID: 32463389 Free PMC article. Review.
-
Interventional treatment strategies for arteriovenous malformations of the mandible and maxilla: 30-year institutional case series.Interv Neuroradiol. 2025 May 21:15910199251343000. doi: 10.1177/15910199251343000. Online ahead of print. Interv Neuroradiol. 2025. PMID: 40398476 Free PMC article.
-
In Vitro Quantification of the Radiopacity of Onyx during Embolization.Neurointervention. 2017 Mar;12(1):3-10. doi: 10.5469/neuroint.2017.12.1.3. Epub 2017 Mar 6. Neurointervention. 2017. PMID: 28316864 Free PMC article.
-
State of the Art in the Role of Endovascular Embolization in the Management of Brain Arteriovenous Malformations-A Systematic Review.J Clin Med. 2022 Dec 4;11(23):7208. doi: 10.3390/jcm11237208. J Clin Med. 2022. PMID: 36498782 Free PMC article. Review.
-
Transarterial Embolization for the Management of Brain Arteriovenous Malformations: A Systematic Review.J Neuroendovasc Ther. 2025;19(1):2024-0049. doi: 10.5797/jnet.ra.2024-0049. Epub 2024 Sep 27. J Neuroendovasc Ther. 2025. PMID: 40018288 Free PMC article. Review.
References
-
- Boulos AS, Levy EI, et al. Evolution of neuroendovascular intervention: A review of advancement in device technology. Neurosurgery. 2004;54:438–453. - PubMed
-
- Florio F, Lauriola W, et al. Endovascular treatment of intracranial arterio-venous malformations with Onyx embolization: preliminary experience. Radiol Med. 2003;106:512–520. - PubMed
-
- Howington JU, Kerber CW, et al. Liquid embolic agents in the treatment of intracranial arteriovenous malformations. Neurosurg Clin N Am. 2005;16:355–363. - PubMed
-
- Jahan R, Murayama Y, et al. Embolization of arteriovenous malformations with Onyx: clinicopathological experience in 23 patients. Neurosurgery. 2001;48:984–985. - PubMed
-
- Song D, Leng B, et al. Onyx in the treatment of large and giant aneurysms and arteriovenous malformations. Chines Medical Jounal. 2004;117:1869–1872. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
