

Thoracic metastasectomy for adoptive immunotherapy of melanoma: a single-institution experience
- PMID: 20584535
- PMCID: PMC7241866
- DOI: 10.1016/j.jtcvs.2010.05.020
Thoracic metastasectomy for adoptive immunotherapy of melanoma: a single-institution experience
Abstract
Objectives: Although refractory to chemotherapy, metastatic melanoma may respond to adoptive immunotherapy. As novel treatments evolve, surgeons may be asked to perform metastasectomy not only for palliation or potential cure but also for isolation of tumor-infiltrating lymphocytes. This study was undertaken to examine outcomes of patients with melanoma undergoing thoracic metastasectomy in preparation for investigational immunotherapy.
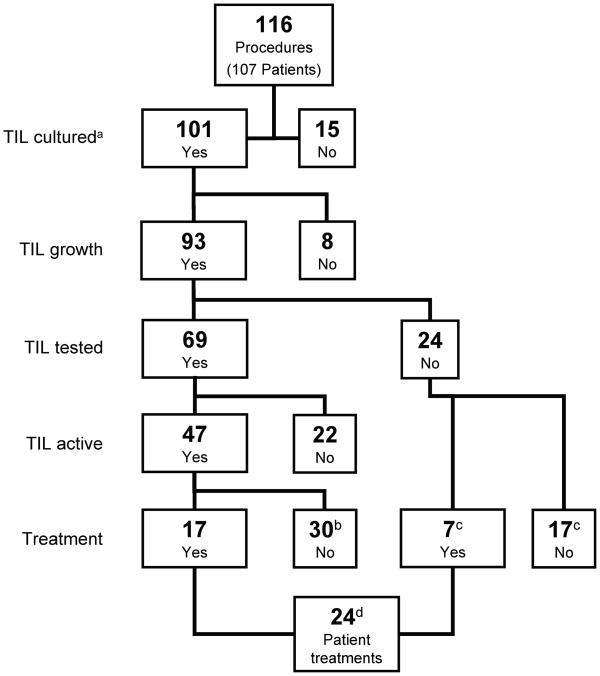
Methods: A retrospective review identified 107 consecutive patients who underwent 116 thoracic metastasectomy procedures from April 1998 to July 2009. Indications for surgical intervention included procurement of tumor-infiltrating lymphocytes, rendering of patients to no evaluable disease status, palliation, and diagnosis. Response Evaluation Criteria in Solid Tumors criteria were used to assess tumor response.
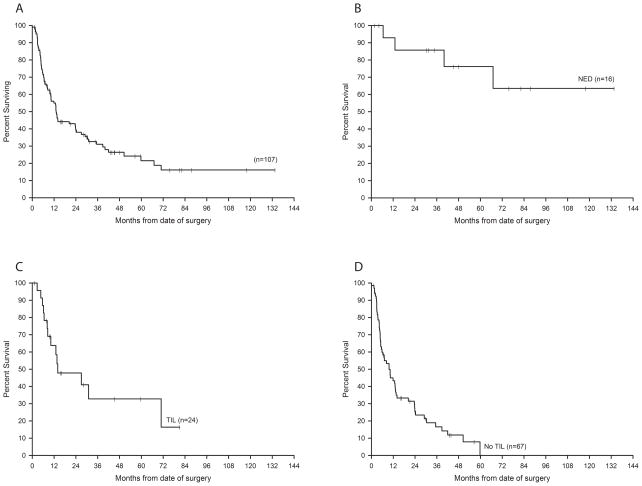
Results: Thoracotomy, lobectomy, and video-assisted thoracoscopic surgery with nonanatomic resection were the most common procedures. Major complications included 1 death and 1 coagulopathy-induced hemothorax. Seventeen patients were rendered to no evaluable disease status. Virtually all patients with residual disease had tumor specimens cultured for tumor-infiltrating lymphocytes; approximately 70% of tumor-infiltrating lymphocyte cultures exhibited antitumor reactivity. Of the 91 patients with residual or recurrent disease, 24 (26%) underwent adoptive cell transfer of tumor-infiltrating lymphocytes, of whom 7 exhibited objective responses (29% response rate and 8% based on intent to treat). Rapid disease progression precluded tumor-infiltrating lymphocyte therapy in most cases. Actuarial 1- and 5-year survival rates for patients rendered to no evaluable disease status or receiving or not receiving tumor-infiltrating lymphocytes were 93% and 76%, 64% and 33%, and 43% and 0%, respectively.
Conclusions: Relatively few patients currently having thoracic metastasectomy undergo adoptive cell transfer. Continued refinement of tumor-infiltrating lymphocyte expansion protocols and improved patient selection might increase the number of patients with melanoma benefiting from these interventions.
Published by Mosby, Inc.
Conflict of interest statement
Conflicts of interest: None
Figures
Similar articles
-
Minimally invasive liver resection to obtain tumor-infiltrating lymphocytes for adoptive cell therapy in patients with metastatic melanoma.World J Surg Oncol. 2012 Jun 22;10:113. doi: 10.1186/1477-7819-10-113. World J Surg Oncol. 2012. PMID: 22726267 Free PMC article.
-
Treatment of metastatic uveal melanoma with adoptive transfer of tumour-infiltrating lymphocytes: a single-centre, two-stage, single-arm, phase 2 study.Lancet Oncol. 2017 Jun;18(6):792-802. doi: 10.1016/S1470-2045(17)30251-6. Epub 2017 Apr 7. Lancet Oncol. 2017. PMID: 28395880 Free PMC article. Clinical Trial.
-
Adjuvant adoptive immunotherapy with tumour-infiltrating lymphocytes and modulated doses of interleukin-2 in 22 patients with melanoma, colorectal and renal cancer, after radical metastasectomy, and in 12 advanced patients.Cancer Immunol Immunother. 1998 Jun;46(4):185-93. doi: 10.1007/s002620050477. Cancer Immunol Immunother. 1998. PMID: 9671141 Free PMC article.
-
Adoptive T-Cell Therapy in Melanoma: How This Will Impact Surgical Practice and the Role of Surgeons.Surg Oncol Clin N Am. 2025 Jul;34(3):423-436. doi: 10.1016/j.soc.2025.01.002. Epub 2025 Feb 27. Surg Oncol Clin N Am. 2025. PMID: 40413008 Review.
-
Report from the European Society of Thoracic Surgeons database 2019: current surgical practice and perioperative outcomes of pulmonary metastasectomy.Eur J Cardiothorac Surg. 2021 May 8;59(5):996-1003. doi: 10.1093/ejcts/ezaa405. Eur J Cardiothorac Surg. 2021. PMID: 33230525 Review.
Cited by
-
Minimally invasive liver resection to obtain tumor-infiltrating lymphocytes for adoptive cell therapy in patients with metastatic melanoma.World J Surg Oncol. 2012 Jun 22;10:113. doi: 10.1186/1477-7819-10-113. World J Surg Oncol. 2012. PMID: 22726267 Free PMC article.
-
Metastasectomy for Tumor-Infiltrating Lymphocytes: An Emerging Operative Indication in Surgical Oncology.Ann Surg Oncol. 2018 Feb;25(2):565-572. doi: 10.1245/s10434-017-6266-8. Epub 2017 Nov 29. Ann Surg Oncol. 2018. PMID: 29188500 Free PMC article.
-
Surgical Considerations for Tumor Tissue Procurement to Obtain Tumor-Infiltrating Lymphocytes for Adoptive Cell Therapy.Cancer J. 2022 Jul-Aug 01;28(4):285-293. doi: 10.1097/PPO.0000000000000608. Cancer J. 2022. PMID: 35880938 Free PMC article. Review.
-
Metastasectomy Following Immunotherapy with Adoptive Cell Transfer for Patients with Advanced Melanoma.Ann Surg Oncol. 2017 Jan;24(1):135-141. doi: 10.1245/s10434-016-5537-0. Epub 2016 Sep 16. Ann Surg Oncol. 2017. PMID: 27638681 Free PMC article.
-
Art of TIL immunotherapy: SITC's perspective on demystifying a complex treatment.J Immunother Cancer. 2025 Jan 20;13(1):e010207. doi: 10.1136/jitc-2024-010207. J Immunother Cancer. 2025. PMID: 39837618 Free PMC article. Review.
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Barth A, Wanek LA, Morton DL. Prognostic factors in 1,521 melanoma patients with distant metastases. J Am Coll Surg. 1995;181:193–201. - PubMed
-
- Balch CM, Soong SJ, Gershenwald JE, Thompson JF, Reintgen DS, Cascinelli N, et al. Prognostic factors analysis of 17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol. 2001;19:3622–34. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
